Psycho-Neuro-Immunological Fatigue syndrome (PNIF) – is micronutrient deficiency the clinically relevant link?
Erpenbach K1, Erpenbach AS1, J Seidl H2, Mayer W3
1Institut für Leistungsoptimierung, Lange Heide 38, 50374 Erftstadt, Deutschland
2Immundiagnostik AG, Stubenwald-Alle 8a, 64625 Bensheim, Deutschland
3Lab4More GmbH, Augustenstraße 10, 80333 München, Deutschland
Received Date: July 17, 2025; Accepted Date: July 30, 2025; Published Date: August 16, 2025;
*Corresponding author: Klaus Erpenbach, 1Institut für Leistungsoptimierung, Lange Heide 38, 50374 Erftstadt, Germany; Email: info@im-lot.org
Citation: Erpenbach K, Erpenbach AS, J Seidl H, Mayer W (2024) Psycho-Neuro-Immunological Fatigue syndrome (PNIF) – is micronutrient deficiency the clinically relevant link? Jr Neuro Psycho and Brain Res: JNPBR-214
DOI: 10.37722/JNPABR.2025202
Abstract
Introduction: Haemopyrroluria (HPU), a phenomenon that occurs more frequently in patients with psychiatric disorders such as schizophrenia, depression, ADHD and anxiety, is defined by the detection of hydroxyhempyrrolin-2-one (HPL) in urine. However, the lack of validity and reproducibility of HPL determination in urine has led to a lack of acceptance of HPU in medical science. Nevertheless, these patients exhibit a specific symptom pattern and benefit from a defined micronutrient treatment. The aim of the study is to proof whether this syndrome pattern can be standardized and whether standardized micronutrient supplementation is therapeutically effective.
Methods: 35 patients with psychiatric disorders (ADHD, depression, anxiety) were included in the study and evaluated anamnestically using a prospective standardized questionnaire to create a total score (TS). Various micronutrients were determined in the blood before and after 6 months of standardized micronutrient treatment. The standardized questionnaire was re-evaluated after 6 months.
Results: Of the 35 patients aged 43 ± 15.44 years (25 women/10 men), 21 (60%) participants suffered from depression, 11 (31.4%) from an anxiety disorder and 3 (8.6%) from ADHD. Additional anamnestic symptoms were fatigue (N=35), susceptibility to infections (N=29), irritable bowel syndrome (N=22), insomnia (N=35), Hashimoto’s thyroiditis (N=12) and a family history of neuropsychiatric disorders. The criteria of a Psycho- (N=35: depression, anxiety disorder, ADHD) Neuro- (N=35: insomnia) Immunological (N=35: susceptibility to infections, irritable bowel syndrome, Hashimoto’s thyroiditis) Fatigue syndrome (N=35) were proved in all patients. The levels of all bioavailable B vitamins were deficient. TS was significantly reduced by the standardized micronutrient treatment (TS before vs. after treatment = 9.06±1.83 vs. 1.23±1.02 – p<0.0001). 10 of the 35 (28.6%) patients receiving psychotropic drug medication at the beginning of the study discontinued their medication during the 6-month micronutrient treatment. The 6-month micronutrient treatment led to a highly significant increase in all bioavailable B vitamins, vitamin D3, Q10, selenium and calcium in whole blood.
Conclusion: Patients with neuropsychiatric disorders show additional symptoms that can be summarized as Psycho-Neuro-Immunological Fatigue syndrome (PNIF syndrome) and, if a family history of neuropsychiatric disorders is detected, indicates a genetic cause. The total score is highly suitable for assessing curative micronutrient treatment. Standardized micronutrient treatment was able to compensate these deficiencies within 6 months, wean patients off psychotropic drugs and significantly reduce their symptoms. Case-control studies are necessary to confirm the specificity and sensitivity of the PNIF questionnaire and randomized placebo-controlled treatment studies are necessary to confirm the effectiveness of standardized micronutrient treatment in PNIF patients.
Watch the Article in Motion
1-Minute Overview
Shorts (GERMAN)
More related videos at the bottom of the page…
Introduction:
Pyrroluria (also known as cryptopyrrole, pyrrole or Mauve factor disease) is a controversial disorder and is defined by the detection of elevated levels of pyrroles in the urine (1-4). As early as 1961, Irvine (1) was able to show that in patients with psychiatric disorders (depression, schizophrenia), substances are excreted in the urine that react blue-purple with the Ehrlich reagent and thus became known as “mauve factor” (mauve = mauve-colored, light purple). The chromato-graphic properties of the “mauve factor” corresponded to those of cryptopyrrole (2,4-dimethyl-3-ethylpyrrole) (3). It was assumed that the pyrrole possibly originated from a disturbed synthesis or metabolism of heme and was an indicator of substances causing the psychiatric symptoms in the affected patients. Irvine revised this in 1978 (5), stating that the substance was probably not kryptopyrrole, but 2-hydroxyhemopyrrolen-5-one (hemopyrrollactam = HPL). However, given the long history of identifying elevated HPL and neuropsychiatric disorders, the reproducibility of HPL determination remains controversial (1-6). Also, the biochemical origin of HPL and the mechanism for increased HPL excretion is unknown. According to Warren et al. (Review 2021), numerous studies have attempted to show a link between elevated pyrrole levels and the diagnosis of neuro-psychiatric disorders, but with limited effects (7). Even the most recent study on 96 patients with neuro-psychiatric disorders and HPL determination in urine could not eliminate the lack of scientific acceptance for HPU (8). However, Erpenbach et al. were able to demonstrate that these patients exhibited a specific symptom pattern and benefited from a defined micronutrient treatment (8). The aim of this study is to standardize this specific symptom pattern and to examine whether the controversial HPL diagnosis is avoidable and whether a standardized micronutrient substitution is therapeutically effective?
Methods:
35 patients with psychiatric disorders [ADHD (N=3), depression (N=21), anxiety disorder (N=11)] were included into the study and evaluated anamnestically using a standardized questionnaire (8). Additional symptoms with a frequency of > 80% were defined as main criteria and scored with 2 points each. Additional symptoms with a frequency < 80% were defined as secondary criteria and scored with one point each. Family criteria resulted from the mentions of family members with neuropsychiatric stress and were scored with one point per mention. The total score was calculated from the addition of the main, secondary and family criteria (8). Following written informed consent, various micronutrients were determined in the blood of the study paients before and after 6 months of standardized micronutrient treatment. The standardized questionnaire was re-evaluated after 6 months of treatment.
Total blood trace elements selenium, zinc, copper, manganese, iron, calcium, magnesium (Na-heparin blood) vSe, vZn, vCu, vMn, vFe, vCa, vMg
Trace elements in total blood were determined using induction-coupled mass spectrometry (ICPMS) on a Purkin-Elmer platform (Nexion2000).
Coenzyme Q10 (serum)
The determination of Q10 in serum was carried out using high-performance liquid chromatography (HPLC) with commercial kits (Chromsystems, Gräfelfing, Germany) according to the manufacturer’s instructions (Q10 – Order No. 68000).
Vitamin D 25-OH (serum)
The quantitative determination of 25-OH vitamin D in serum was carried out according to the manufacturer’s instructions using a direct competitive chemiluminescence immunoassay (CLIA) on the Liasion-XL automated laboratory system from Diasorin, Dietzenbach, Germany (Order No. 310600).
bioavailable Vitamin B1, B2, B6, B9, B12
The determination of bioavailable vitamins B1, B2, B6, B9 (folic acid) and B12 was carried out using standardized microbiological test kits from the ID-Vit® product line (Immundiagnostik AG, Bensheim, Germany) in accordance with the manufacturer’s instructions. Specific microorganisms are added to the patient sample in a vitamin-specific deficiency medium. Quantification takes place after incubation using a standard series.
B1 (EDTA total blood): Total blood was pretreated, diluted and added to microtiter plates containing Lactobacillus fermentum. Incubation was carried out at 37°C for 48 h
B2 (serum): Serum samples were pretreated and pipetted onto microtiter plates containing Lactobacillus rhamnosus. Incubation was carried out at 37°C for 72 h.
B6 (serum): Serum was enzymatically pretreated and added to microtiter plates containing Saccharomyces cerevisiae. Growth was measured after 48 h incubation at 30°C.
B9 (folic acid, serum): Serum was pretreated and pipetted onto microtiter plates containing Lactobacillus rhamnosus. After 46-50 h incubation at 37°C the turbidity was determined.
B12 (serum): Serum was pretreated and added to microtiter plates containing Lactobacillus delbrueckii subsp. lactis. Incubation was carried out at 37°C for 46-50 h.
The growth of the microorganisms was quantified via turbidity at 620 nm. The method allows the determination of bioavailable vitamins.
All patients daily took BIONOVELIA B-complex capsules (1-0-1), BIONOVELIA Q10-R liquid (1 tablespoon in the morning), BIONOVELIA K2-200µ/D3-10000IE capsules (1-0-0) [Fagus Pharma, Brühl, Germany].
Statistical analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS) 24 (IBM Corporation, Armonk, NY, USA) and Microsoft Excel 2016 (Microsoft Corporation, Redmond, WN, USA). Quantitative parameters described by mean, median and minimum-maximum values. Pairwise comparisons were performed using the Wilcoxon and non-parametric Mann-Whitney U tests. The Pearson chi-square test was used to determine relationships between categorical variables. In all statistical tests, results were interpreted as statistically significant if p was less than 0.05, with p ≤ 0.01 considered highly significant.
Results:
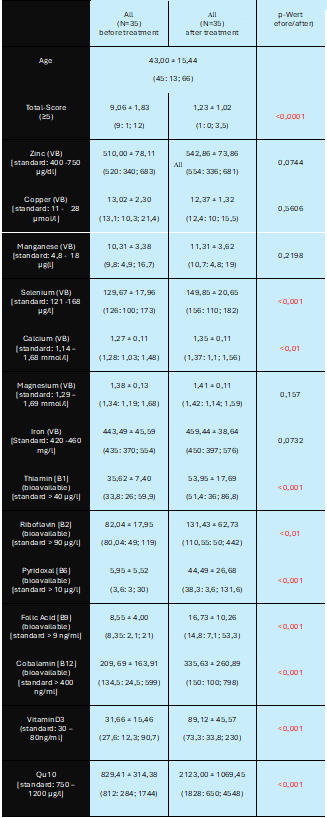
Of the 35 patients aged 43.00 ± 15.44 years (25 women/10 men), 21 (60%) suffered from depression, 11 (31.4%) from an anxiety disorder and 3 (8.6%) from ADHD. Additional anamnestic symptoms (Table 1) were fatigue (patients with depression / anxiety disorder / ADHD = all 100%), susceptibility to infections (71% / 100% / 100%), irritable bowel syndrome (71% / 45% / 67%), insomnia (all 100%), Hashimoto’s thyroiditis (33% / 45% / 0%) and a family history of neuropsychiatric disorders [number in the family: 1(1-4) / 2(1-3) / 1(1-1)]. The total score before treatment was 9.06±1.83 points and consisted of major criteria (5.66±0.76 points), minor criteria (1.97±0.75 points) and family criteria (1.66±0.84 points). The criteria for Psycho- (N=35: depression, anxiety disorder, ADHD) Neuro- (N=35: insomnia) Immunological (N=35: susceptibility to infections, irritable bowel syndrome, Hashimoto’s thyroiditis) Fatigue syndrome (N=35) were proved in all patients (Figure 1). Before micronutrient treatment, the levels of all bioavailable B vitamins [B1=35.62 ± 7.4µg/l, B2=82.04 ± 17.95µg/l, B6=5.95 ± 5.52µg/l, B9=8.55 ± 4.00ng/ml, B12=209.69 ± 163.91ng/ml)] were diminished (Table 2). The vitamin D3 level and the levels of all trace elements in the whole blood (selenium, zinc, calcium, magnesium, copper, manganese, iron) as well as the Q10 value were within the international normal range for all patients before treatment, but not within the therapeutic range of 1200 – 2500 µg/l for Q10.
Figure1: Psycho-Neuro-Immunological Fatigue-Syndrome (criteria)
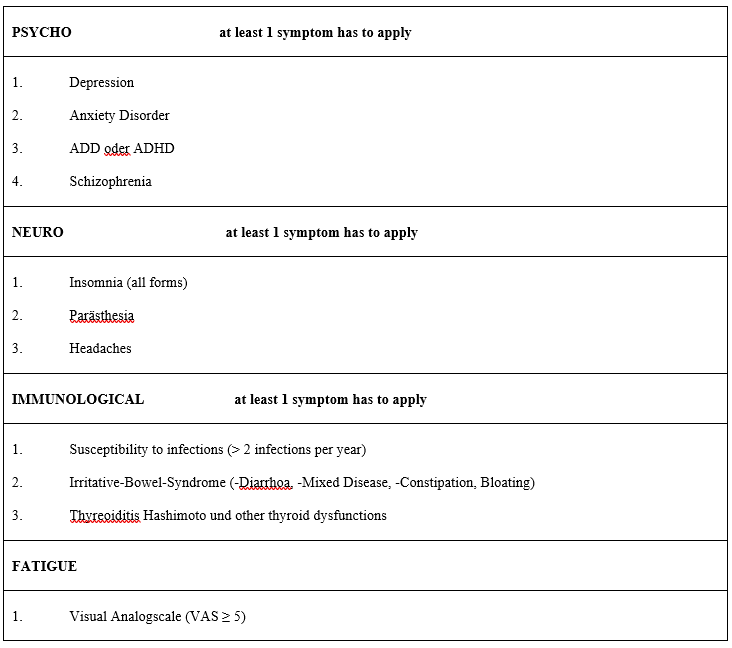
Table 1: Additional symptoms of the study patients in relation to the neuro-psychiatric disorders. N = number, ADHD = attention deficit hyperactivity disorder, VAS = visual analog scale, IBS = irritative Bowel Syndrome, (minimum – maximum)
| ADHD (N=3) | Depression (N=21) | Anxiety (N=11) | |
| Main Criteria (> 80% Nomination) | |||
| Fatigue (≥ VAS = 5) Susceptibility to infections (> 2x per year) | 100% 100% | 100% 71% | 100% 100% |
| Side Criteria (< 80% Nomination) | |||
| IBS (all forms with / without bloating) Insomnia (all forms) Thyreoiditis Hashimoto | 67% 100% 0% | 71% 100% 33% | 45% 100% 45% |
| Family Criteria (Number) | |||
| Relatives with neuro-psychiatric disorders | 1 (1-1) | 1 (1-4) | 2 (1-3) |
TS was significantly reduced by the standardized micronutrient treatment (TS before vs. after treatment = 9.06±1.83 vs. 1.23±1.02 – p<0.0001). 10 of the 35 (29%) patients were receiving psychotropic drug therapy at the beginning of the study (mirtazapine N=6, opipramol N=3, venlafaxine N=1), which could be discontinued during the 6-month micronutrient treatment. The 6-month micronutrient treatment led to a highly significant increase in all bioavailable B vitamins (B1 before vs. after: 35.62±7.40 vs. 53.95±12.69 µg/l – p<0.0001, B2: 82.04±17.95 vs 122.94±67.79 µg/l – p<0.01, B6: 5.95±5.52 vs 44.49±26.68 µg/l – p<0.0001, B9: 8.55±4.00 vs 16.73±10.73 ng/ml – p<0.0001, B12: 209.69±163.91 vs 335.63±260.89 ng/ml -p<0.0001), in vitaminD3 (31. 55±15.46 vs 89.12±45.57 ng/ml – p<0.0001), in Q10 (829.41±314.38 vs 2123.00±1069.45 µg/l – p<0.0001), in selenium (129.67±17.96 vs 149.85±20.65 µg/l – p<0.001) and in calcium (1.27±0.11 vs 1.35±0.11 mmol/l – p<0.01) in total blood. Magnesium, iron, copper, manganese and zinc in total blood remained unchanged under micronutrient treatment (Table 2). No side effects were reported.
Table 2: Demographic characteristics (participants). N = number, (median: minimum; maximum). VB = total blood
Discussion:
Chronic susceptibility to infections, particularly to viruses (especially herpes viruses), progressive fatigue, irritable bowel symptoms, sleep disorders and symptoms of thyroid dysfunction were the most frequently mentioned additional symptoms in our study in patients with neuropsychiatric disorders and confirm the results from our recent HPU study (8).
The repeatability of the symptom pattern: fatigue, neuro-psychiatric disorders with additional neurological and immunological symptoms in our study allows to define a Psycho-Neuro-Immunological Fatigue syndrome (PNIF syndrome) [Fig. 1], which can replace the determination of the disputed HPL complex in urine and can be validly compared for future studies by the reproducible total score of this PNIF syndrome.
The term Psycho-Neuro-Immune-Endocrinology (PNIE) was first described in 1936, although the effects of psychology on health have been known since ancient times and documented in various cultures. It encompasses the study of the interactions between various psychological factors and physiological processes such as neuronal, endocrine and immune responses (9-11). Thus, the discipline addresses all four clinical areas – psychology, nervous system, immunology and endocrinology – in various combinations and may be able to explore the cause and development of many disease whose etiology were previously unknown (10,12-13). Psychology is the study of mind and behavior and their interactions, expressions, etc. The altered function of the nervous system, whether central or peripheral or both, affects both the body and the mind (12,14-15).
Immunology studies the development and functioning of the body’s defense mechanisms against invaders. While an dysfunction of one or more body systems can make a person susceptible to infectious agents, uncontrolled or excessive activity of these systems can also lead to serious illness (12,15). The term PsychoNeuroImmunology (PNI) describes the interactions between an individual’s emotional states, nervous system functions and immune system, and the consequences of such interactions (9,15). Endocrinology deals with the coordinated effects of various hormones on metabolism, energy production, growth, reproduction, stress, mood, etc., and various clinical conditions can result from altered hormone secretion or function (9,14-15). The field of psycho-neuro-immuno-endocrinology is concerned with identifying the mechanisms of mind-body interaction (9,12,16) and the effects of mental state on physical health. However, the reverse effects (influence of physical state on mental health) occur equally (17). In our study, Psycho-Neuro-Immunology is expanded to include Fatigue to form PNIF syndrome. The term PSYCHO is defined here by depression or anxiety disorder or ADHD, the term NEURO by insomnia, the term IMMUNO by chronic susceptibility to infection, irritable bowel syndrome or Hashimoto’s thyroiditis, and FATIGUE stands for itself. What all diseases have in common is the need for optimal micronutrient concentrations: Bioavailable vitamin B6 and magnesium together with tryptophan and thyrosine are required for the production of important neurotransmitters such as serotonin (against depression), dopamine (regulates concentration and coordination), adrenaline / noradrenaline (regulates stress tolerance and aggressiveness) and melatonin (induces sleep) (18) [Fig.2]. Almost all trace elements are needed to maintain immune function against viruses (zinc, selenium), to protect the thyroid gland (selenium) and to eliminate oxidative radicals in the cell via superoxide dismutases (copper, manganese and zinc-dependent) and glutathione peroxidases (selenium-dependent) (19) [Fig.2]. Almost all bioavailable B vitamins are required in the gut to maintain a healthy microbiome via the optimization of butyric acid-producing bacteria and the regulation of intestinal serotonin, tryptophan and gamma-amino-butyric acid (GABA) (20-21) [Fig.2]. B vitamins, Q10 and iron as well as magnesium are important mitotropic micronutrients for cellular energy production in the mitochondrion. Vitamin D3 regulates immune function by downregulating various cytokines (19) and in combination with vitaminC and Q10 it reduces the levels of all autoantibodies against G-protein-coupled receptors which are involved in Chronic-Fatigue-Syndrome and in LONG- and POST-COVID-Syndrome (22) [Fig.2]. Various enzymes regulate the synthesis and metabolism of all neurotransmitters and influence the development of various neuropsychiatric disorders via polymorphisms. Rambaud et al. confirmed that oxidative stress is not only associated with schizophrenia but also with other neuropsychiatric and metabolic disorders (23). Our own genetic studies in patients with neuropsychiatric disorders (ADHD, depression, anxiety disorder) and increased HPL excretion in urine show the following changes: in decreasing frequency COMT (N=4), MTHFR (N=3), TPH1 (N=2), MAOA (N=2), IL6 (N=1), eNOS (N=1) and thus also indicate the possibility of an inflammatory-oxidative process (8). COMT (catecholamine O-methyl transferase), which is primarily responsible for the rapid degradation of dopamine and noradrenaline and requires various cofactors (B1, B2, B6, B9, B12, Q10), leads to panic disorders in the active form VAL158, particularly in women (24). Genes of tryptophan hydroxylase (TPH), the limiting enzyme of serotonin synthesis, which catalyzes the hydroxylation of tryptophan to 5-hydroxytryptophan (5-HTP) and requires vitamin B9 (folic acid), magnesium and vitamin C as a cofactor, favor the development of depressive disorders in the case of genetic changes (25). Monoamine oxidase A (MAO-A), the determining enzyme of serotonin metabolism, requires vitamin B2 as a cofactor and leads to aggressive behavior in the case of genetic changes (26). The interleukin-6 (IL6) and eNOS polymorphisms emphasize the component of oxidative stress as a trigger of neuropsychiatric disorders and require a high antioxidant capacity of selenium, zinc, vitamin C and Q10 as counterparts [Fig.2]. Common to all genetic triggers is the dependence on all bioavailable B vitamins and trace elements (27).
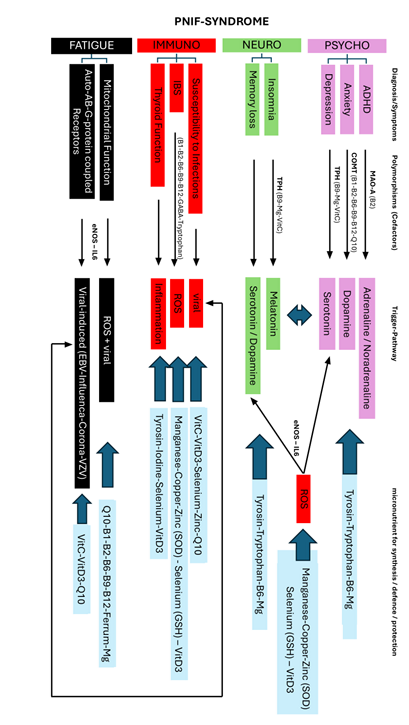
Figure 2: Flow-Chart Psycho-Neuro-Immuno-Fatigue (PNIF)-Syndrome: Link between diagnosis / symptoms and micro nutrients. ADHD = Attention Deficit Hyperactivity Disorder, IBS = Irritative Bowel Syndrome, AB = Autoantibody, MAO-A = Monoaminoxidase-A, COMT = Catechol-O-Methyltransferase, TPH = Tryptophanhydroxylase, eNOS = endothelial nitric oxide synthase, IL6 = Interleukin 6, ROS = reactive oxygen species, EBV = Ebstein-Barr-Virus, VZV = Varicella-Zoster-Virus, SOD = Superoxiddismutase, GSH = Glutathionperoxidase, Mg = Magnesium
In our study, the concentrations of all bioavailable B vitamins (B1, B2, B6, B9, B12) were deficient in the micronutrient analysis prior to treatment. However, the concentrations of all trace elements in the total blood (selenium, zinc, calcium, magnesium, copper, manganese, iron) and the Q10 level were within the normal range in all participants before treatment. Our study group was recently able to confirm the same results in patients with neuropsychiatric disorders and increased HPL excretion (8). Mikirova (28) was also unable to detect any trace element deficiencies in total blood (copper, manganese, zinc, iron, selenium) in her patients with neuropsychiatric disorders (ADHD, schizophrenia, bipolar disorder, depression) and increased HPL excretion. These results confirm the results from our HPU study and the inferiority of therapy with pyridoxal-5-phosphate, zinc and magnesium alone in the treatment of patients with neuro-psychiatric disorders (8).
Conclusion:
The clinically relevant link for all symptoms of Psycho-Neuro-Immuno-Fatigue syndrome (PNIF syndrome) appears to be micronutrient deficiency (especially of the bioavailable, active B vitamins and all intracellular trace elements). Further research is required to clarify the discrepancy between the serological B-vitamin levels in serum (inactive form) and the bioavailable B-vitamins (active form) as well as the trace elements in serum and total blood. Determination of the scientifically controversial hemopyrroles in urine does not appear to be necessary in the future to prove PNIF syndrome. There is clear and replicable clinical evidence that patients with a neuro-psychiatric disease have specific accompanying symptoms, which can be defined as a Psycho-Neuro-Immunological Fatigue syndrome (PNIF syndrome) and successfully treated with a standardized micronutrient regimen. Double-blind, placebo-controlled studies are needed to prove the efficacy of micronutrient treatment in patients with PNIF syndrome.
References:
- Irvine D. Apparently non-indolic Ehrlich-positive substances related to mental illnesses. J Neuropsychiatry 1961:292–305
- Hoffer A. The discovery of kryptopyrrole and its importance in diagnosis of biochemical imbalances in schizophrenia and in criminal behavior. J Orthomol Med 1995;10:3–6
- Irvine D, Bayne W, Miyashita H. Identification of kryptopyrrole in human urine and its relation to psychosis. Nature 1969;224(5221):811–883
- McGinnis W, Audhya T, Walsh W, et al. Discerning the mauve factor, part 1. Altern Ther Health Med 2008;14:40–50
- Irvine D. Hydroxy-hemopyrrolenone, not kryptopyrrole, in the urine of schizophrenics and porphyrics. Clin Chem 1978;24:2069–2070
- Pfeiffer CC, Sohler A, Jennery C, et al. Treatment of pyroluric schizophrenia with large doses of pyridoxine and a dietary supplement of zinc. J Orthomol Psychiatr 1974;3:292–300
- Warren B, Sarris J, Mulder RT, Rucklidge JJ. Pyroluria: Fact or Fiction? J. Altern. Complement. Med. 2021, 27, 407–415
- Erpenbach K, Erpenbach AS, Kamsteeg J, Seidl H, Mayer W, Baumeister-Jesch L. Neuropsychiatric Disorders and Hemopyrollactamuria (HPU) – fact or fiction? J Neurol Psych Brain Research 2025, 207 (1), 1-14
- Murray MT, Nowicki J. Immune System Support. In: Pizzorno JE, Murray MT (Eds.), Textbook of Natural Medicine (5th edn.), Churchill Livingstone. 2020; 1009-1016.e2, DOI:10.1016/B978-0-323-43044-9.00136-9
- Solomon GF. The development and history of psychoneuroimmunology, the link between religion and health: psychoneuroimmunology and the faith factor. Online Education, 2010; Oxford Academic, DOI:10.1093/acprof:oso/9780195143607.003. 0003
- Zachariae R. Psychoneuroimmunology: a bio-psycho-social approach to health and disease. Scand J Psychol. 2009; 50(6):645-651, DOI:10.1111/j.1467-9450.2009. 00779.x.
- Slavich GM. Psychoneuroimmunology of stress and mental health. In: Harkness K, Hayden EP. (Eds.), The Oxford handbook of stress and mental health. 2019; Oxford University Press, New York, DOI:10.1093/oxfordhb/9780190681777.013.24.
- González-Díaz SN, Arias-Cruz A, Elizondo-Villarreal B, Monge-Ortega OP. Psychoneuroimmunoendocrinology: clinical implications. World Allergy Organizati J. 2017; 10:19, DOI:10.1186/s40413-017-0151-6.
- Bower JE, Kuhlman KR. Psychoneuroimmunology: An introduction to immune-to-brain communication and its implications for clinical psychology. Annu Rev Clin Psychol. 2023; 19:331-359, DOI:10.1146/annurev-clinpsy-080621-045153.
- Seladi-Schulman J. Understanding psychoneuroimmunology: What is psychoneuroimmunology? 2018; https://www.healthline.com/health/psychoneuro-immunology
- Jiménez JA, Mills PJ, Behavioral Medicine. In: Ramachandran VS (Ed.), Encyclopedia of Human Behavior (2nd edn.), 2012; 311-318. Academic Press, DOI:10.1016/B978-0-12-375000-6.00057-4.
- Carroll K. Psychoneuroimmunology examples. 2023; https://study.com/academy/lesson/what-is-psychoneuroimmunology-definition-lesson.html.
- Ebadi M, Gessert CF, Al-Sayegh. Drug-Pyridoxal Phosphate Interactions. Rev Drug Metabol Interact 1982; 4(4): 289-332
- Erpenbach K. Mikronährstoffmangel bei chronischen Entzündungen (Silent Inflammation). In: Tiller FW, Mayer W (eds), Silent Inflammation, 2024 (1.Auflage): 130-172 ML Verlag Kulmbach
- Seidl H, Bastian S. Das Reizdarmsyndrom – Pathomechanismen und innovative Stuhldiagnostik im Focus der Darm-Hirn-Achse. OM&Ernährung 2023; 182:F104-F113
- Mishima Y, Ishihara S. Enteric Microbiota-Mediated Serotonergic Signaling in Pathogenesis of Irritable Bowel Syndrome. Int J Mol Sci 2021; 22: 10235, doi.org(10.3390/ijms221910235
- Erpenbach K, Erpenbach AS, Mayer W, Weck M. SARS-CoV-2-Omicron-variant induced COVID-19-infection in unvaccinated and vaccinated patients: Impact on immune response, symptomatology, and risk of POST-COVID syndrome. J Immun Res Rep. 2023; 3 (1): 1-8
- Rambaud V, Marzo A, Chaumette B. Oxidative Stress and Emergence of Psychosis. Antioxidants 2022, 11, 1870
- Rothe C, Koszycki D, Bradwejn J, King N, Deluca V, Tharmalingam S, Macciardi F, Deckert J, Kennedy JL. Association of the Val158Met Catechol O-Methyltransferase Genetic Polymorphism with Panic Disorder. Neuropsychopharmacology 2006; 31, 2237–2242
- Zhang X, Gainetdinov RR, Beaulieu JM, Sotnikova TD, Burch LH, Williams RB, Schwartz DA, Krishnan KRR, Caron MC. Loss-of-Function Mutation in Tryptophan Hydroxylase-2 Identified in Unipolar Major Depression Neuron 2005; 45, 11–16
- McDermotta R, Tingleyb D, Cowdenc J, Frazzettod G, Johnson DDP. Monoamine oxidase A gene (MAOA) predicts behavioral aggression following provocation. PNAS 2009; 106 (7): 2118 –2123
- Aly J, Engmann O. The way to a human’s brain goes through their stomach: dietary factors in major depressive disorder. Frontiers in Neuroscience. 2020; 14. https://doi.org/10.3389/fnins.2020.582853
- Mikirova, N. Clinical Test of Pyrroles: Usefulness and Association with Other Biochemical Markers. Clin. Med. Rev. Case Rep. 2015; 2: 27