Intravenous Autologous Adipose‑Derived Expanded Mesenchymal Stem Cell Therapy in Inclusion Body Myositis: A First‑in‑Human Case Report
Hassan Mubark*
DOI: 10.37722/AOASM.2026101
Abstract
Background:
Inclusion body myositis (IBM) is the most common acquired inflammatory myopathy in individuals over 50 years of age and remains refractory to conventional immunosuppressive and disease-modifying therapies. Its pathogenesis reflects a multifactorial process involving chronic cytotoxic T-cell–mediated inflammation, protein dyshomeostasis, mitochondrial dysfunction, and progressive muscle fiber degeneration. To date, human cell-based studies in IBM have been confined to localized intramuscular administration of adipose-derived mesenchymal stem cells, with no published reports describing systemic intravenous cell therapy.
Case Presentation:
We report a first-in-human case of intravenous autologous adipose-derived, purified, culture-expanded mesenchymal stem cell (MSC) therapy in a 70-year-old male with biopsy-confirmed IBM and a 13-year history of progressive muscle weakness. The patient received three intravenous infusions of 100 million MSCs administered at six-week intervals. Treatment was well tolerated with no immediate or delayed adverse events. Clinically, the patient demonstrated meaningful improvement in upper-limb muscle strength and bulk, cessation of recurrent falls, and stabilization of functional decline. Biochemically, serum creatine kinase (CK) levels, which had remained persistently elevated prior to treatment (281–384 U/L; reference range 60–220 U/L), normalized to 213 U/L nine months after treatment initiation.
Conclusion:
This first-in-human systemic case provides preliminary evidence supporting the feasibility, safety, and potential biological activity of intravenous mesenchymal stem cell therapy in inclusion body myositis. Compared with localized intramuscular delivery, systemic administration may confer advantages by enabling global immunomodulation and broader disease modification. These findings support the need for future randomized controlled trials to formally evaluate efficacy, optimal dosing, and treatment durability.

Watch the Article in Motion
Information Board
ISSN: 2641-6859
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Language:English
Impact Factor: 4.9
Keywrods: Inclusion body myositis; mesenchymal stem cells; MSCs; adipose‑derived stem cells; intravenous cell therapy; immunomodulation; regenerative medicine.
Introduction
Inclusion body myositis (IBM) is a relentlessly progressive inflammatory myopathy characterized by asymmetric weakness affecting both proximal and distal muscle groups, particularly the quadriceps and finger flexors. It is the most common acquired myopathy in adults over the age of 50 and is associated with progressive disability, frequent falls, dysphagia, and eventual loss of independence [1]. Unlike other idiopathic inflammatory myopathies, IBM responds poorly to corticosteroids, immunosuppressive agents, and biologic therapies [2,3].
IBM is uniquely refractory to conventional immunomodulatory treatments because its pathogenesis reflects the coexistence of immune-mediated cytotoxicity and intrinsic degenerative myofiber pathology. Persistent CD8⁺ cytotoxic T-cell invasion of non-necrotic muscle fibers occurs alongside abnormal protein aggregation, impaired autophagy, mitochondrial dysfunction, and age-related immunosenescence. This complex and self-reinforcing disease biology renders single-pathway immunosuppression largely ineffective and distinguishes IBM from other inflammatory myopathies that are more treatment responsive.
Histopathologically, IBM is defined by endomysial inflammation with CD8⁺ T-cell invasion of intact muscle fibers in conjunction with degenerative features such as rimmed vacuoles, misfolded protein accumulation, mitochondrial abnormalities, and disrupted autophagic clearance [4]. The convergence of inflammatory and degenerative mechanisms has complicated therapeutic development and contributes to the repeated failure of pharmacologic interventions [5].
Multiple randomized controlled trials evaluating corticosteroids, methotrexate, azathioprine, interferon-β, tumor necrosis factor inhibitors, and other immunomodulatory agents have failed to demonstrate sustained clinical benefit [6]. Intravenous immunoglobulin has shown at best transient or modest effects without altering long-term disease progression [7]. More recent efforts targeting protein homeostasis and cellular stress pathways, including heat-shock response modulators such as arimoclomol, have similarly failed to demonstrate meaningful clinical efficacy in controlled trials [8]. Collectively, these findings underscore the urgent need for therapeutic strategies capable of addressing both immune dysregulation and degenerative pathology.
Mesenchymal stem cells (MSCs) possess immunomodulatory, anti-inflammatory, anti-fibrotic, and trophic properties. They suppress cytotoxic T-cell activity, modulate macrophage polarization, downregulate pro-inflammatory cytokines, and promote tissue repair primarily through paracrine mechanisms [9,10]. These multimodal effects render MSCs particularly attractive in IBM, where immune-mediated injury and intrinsic muscle degeneration coexist and evolve in parallel.
To date, human stem-cell–based investigations in IBM have been limited to localized intramuscular administration of adipose-derived regenerative cells, primarily designed to assess safety rather than efficacy. A Phase I open-label study conducted at Kansas University evaluated the safety of intramuscular adipose-derived cell injections into forearm and thigh muscles of IBM patients, demonstrating feasibility and tolerability but without evidence of systemic disease modification [11]. Importantly, no peer-reviewed human studies have evaluated intravenous stem cell therapy in IBM, leaving the potential role of systemic immunomodulation unexplored. We therefore report a first-in-human case exploring intravenous autologous adipose-derived expanded MSC therapy as a novel systemic therapeutic approach.
Case Presentation and therapeutic protocol
A 70‑year‑old male with biopsy‑confirmed sporadic inclusion body myositis (IBM) presented with a 13‑year history of progressive muscle weakness. Initial symptoms involved the quadriceps muscles, followed by progressive distal lower‑limb and upper‑limb weakness, recurrent falls, and difficulty rising from seated positions. Upper‑limb involvement became increasingly functionally limiting over time. Despite prolonged supportive and conservative management, disease progression continued unabated.
Over the four years preceding stem cell therapy, serum creatine kinase (CK) levels monitored by the treating neurologist remained persistently elevated, ranging from 281 to 384 U/L (reference range 60–220 U/L). Progressive knee hyperextension secondary to IBM-related neuromuscular impairment resulted in marked joint instability, abnormal mechanical loading across both knees, and accelerated bilateral osteoarthritic degeneration. This was accompanied by a stepwise decline in functional mobility and ambulation capacity, such that the patient became dependent on a rollator for mobility.
Given the immune‑mediated pathophysiology of IBM and lack of effective disease‑modifying therapies, a systemic immunomodulatory strategy using experimental autologous adipose‑derived, purified, culture‑expanded MSCs was undertaken following informed consent. Abdominal adipose tissue was harvested by a qualified plastic surgeon. MSCs were isolated and culture‑expanded in a biological laboratory according to an approved protocol. Lipoaspirate was enzymatically digested using collagenase, and the stromal vascular fraction was isolated by density‑gradient centrifugation. Cells were cultured in Dulbecco’s Modified Eagle Medium supplemented with human platelet lysate and expanded to approximately 90% confluence before cryopreservation.
On the day of administration, cells were thawed, washed, filtered, and resuspended in Hartmann’s solution with human platelet lysate. Cell counts and viability were confirmed prior to infusion. The patient received three intravenous infusions of 100 million MSCs, administered initially nine months prior to reporting and subsequently at six‑week intervals. Each infusion was delivered in a monitored medical facility under continuous one‑to‑one clinician supervision. Prolonged fasting for several hours, without fluid restriction, was undertaken prior to each infusion as a strategy intended to potentially enhance mesenchymal stem cell activity.
All infusions were well tolerated, with no immediate or delayed adverse events observed. Following each infusion, adjunctive photobiomodulation laser therapy and light-resistance physiotherapy were implemented with the aim of supporting mesenchymal stem cell activity and providing transient anti-inflammatory effects. A couple of months after completion of MSC therapy, the patient underwent platelet-rich plasma injections for symptomatic bilateral knees osteoarthritis and was prescribed custom knee bracing to enhance joint stability.
Clinical outcomes were assessed using physician-evaluated muscle strength and functional performance, including grip strength, elbow flexion strength, ability to rise from a seated position, and fall frequency, supported by serial photographic documentation during in-person and telehealth follow-up. Laboratory outcomes were evaluated using repeated post-treatment serum creatine kinase (CK) measurements.
Clinically, the patient showed a gradual but moderate improvement in upper-limb strength and functional capacity, with improved ability to rise from a seated position and complete resolution of recurrent falls. Mild improvement in lower-limb function was noted. The patient reported subjective improvement in upper-limb strength, stating: “I am very pleased with the improved muscle strength in my arms. I can push myself up from either lying down or sitting much better than several months ago. Greater strength in the legs is harder to quantify.”
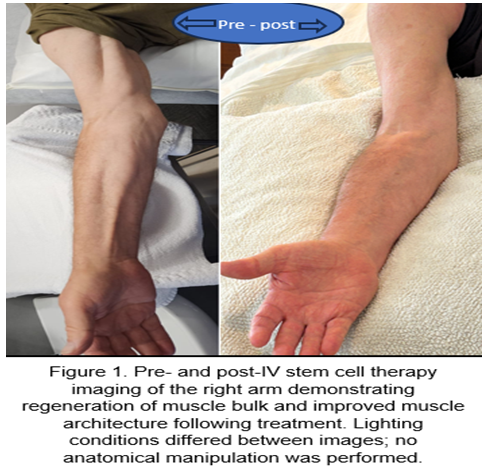
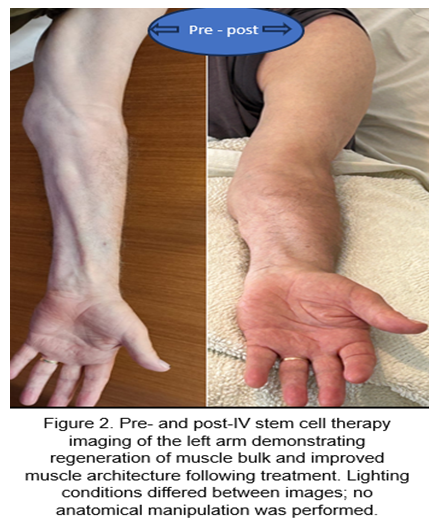
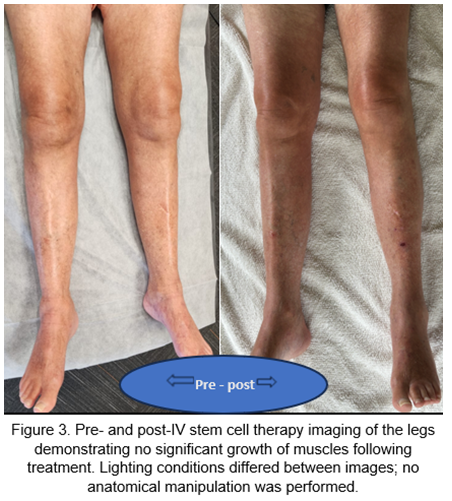
Physical and telehealth with picture provided follow‑ups demonstrated improved upper‑limb muscle bulk and strength, particularly grip strength and elbow flexion (Figures 1 and 2). Lower‑limb muscle bulk did not significantly increase (Figures 1); however, functional decline appeared to stabilize. Eight months after the first infusion, serum CK normalized to 213 U/L.
Discussion
IBM remains one of the most treatments‑refractory inflammatory myopathies, with repeated failures of immunosuppressive and disease‑modifying therapies underscoring the inadequacy of conventional approaches [12]. Persistent cytotoxic T‑cell infiltration despite immunosuppression suggests a self‑sustaining immune process resistant to pharmacologic blockade [13,14].
Beyond inflammation, defective proteostasis, impaired autophagy, mitochondrial abnormalities, and endoplasmic reticulum stress contribute substantially to disease progression [15]. Therapies targeting a single pathogenic pathway are therefore unlikely to meaningfully alter disease trajectory.
MSCs represent a multimodal therapeutic platform capable of addressing immune dysregulation and degeneration simultaneously. MSCs inhibit CD8⁺ T‑cell proliferation, downregulate pro‑inflammatory cytokines, and promote regulatory immune phenotypes through paracrine mechanisms [16]. Preclinical studies demonstrate that MSCs reduce inflammation and enhance muscle regeneration even in the absence of long‑term engraftment [17,18].
The present case should be interpreted in the context of prior human stem cell studies in IBM, which have been restricted to localized intramuscular delivery, a Phase I safety study from Kansas University investigated intramuscular autologous adipose‑derived regenerative cell injections in IBM patients, focusing on feasibility and short‑term safety outcomes [11]. While localized delivery may address focal pathology, IBM is a diffuse systemic immune‑mediated disease. Intravenous MSC administration offers the theoretical advantage of global immunomodulation via effects on circulating immune cells, lymphoid organs, and widespread muscle inflammation.
The present case should be interpreted in the context of prior human stem cell studies in IBM, which have been restricted to localized intramuscular delivery. Intravenous MSC administration offers the theoretical advantage of global immunomodulation via effects on circulating immune cells, lymphoid organs, and widespread muscle inflammation.
In this case, intravenous MSC therapy was well tolerated and associated with meaningful clinical improvement, functional stabilization, cessation of falls, and normalization of CK. Although lower‑limb muscle bulk did not significantly increase, this likely reflects advanced irreversible degeneration. In the context of IBM’s relentlessly progressive course, disease stabilization itself represents a clinically meaningful outcome.
Limitations of this report include its single-patient design and the absence of standardized quantitative strength assessments. Nonetheless, as a first-in-human systemic intravenous application, the therapy demonstrated an acceptable safety profile, consistent with evidence from large-scale clinical cohorts evaluating intravenous mesenchymal stromal cell administration [19] and established preliminary feasibility. Collectively, these observations provide a strong biological and clinical rationale for rigorously designed controlled trials to define optimal dosing strategies, infusion frequency, immunological biomarkers, and objective functional outcome measures.
Conclusion
This first‑in‑human case demonstrates that intravenous autologous adipose‑derived expanded MSC therapy is feasible, safe, and biologically active in inclusion body myositis. Systemic immunomodulatory cell therapy may represent a promising therapeutic avenue in this otherwise treatment‑refractory disease and warrants further controlled clinical investigation.
Patient Consent: Written informed consent was obtained for publication.
Acknowledgements: The authors thank the patient for consenting to share his case in support of advancing regenerative science. The author also acknowledges his wife, Zahraa Jasim, for her administrative support and encouragement in the innovative field of regenerative medicine.
References
- Greenberg SA. Inclusion body myositis: clinical features and pathogenesis. Nat Rev Rheumatol. 2019;15(5):257–272.
- Campanilho-Marques R, Fonseca JE, Machado PM. Treatment of idiopathic inflammatory myopathies. Joint Bone Spine. 2025 Dec;92(6):105932.
- Skolka MP, Naddaf E. Exploring challenges in the management and treatment of inclusion body myositis. Curr Opin Rheumatol. 2023 Nov 1;35(6):404-413.
- Askanas V, Engel WK, Nogalska A. Sporadic inclusion-body myositis: a degenerative muscle disease associated with aging, impaired muscle protein homeostasis and abnormal mitophagy. Biochim Biophys Acta. 2015 Apr;1852(4):633–643.
- Machado PM, Dimachkie MM, Barohn RJ. Sporadic inclusion body myositis: new insights and potential therapy. Curr Opin Neurol. 2014;27(5):591–598.
- Naddaf E, Barohn RJ, Dimachkie MM. Inclusion body myositis: update on pathogenesis and treatment. Neurotherapeutics. 2018 Oct;15(4):995–1005.
- Dobloug C, Walle-Hansen R, et al. Long-term follow-up of sporadic inclusion body myositis treated with intravenous immunoglobulin: a retrospective study of 16 patients. Clin Exp Rheumatol. 2012 Nov–Dec;30(6):838–842.
- Machado PM, McDermott MP, Blaettler T, Sundgreen C, Amato AA, Ciafaloni E, et al. Safety and efficacy of arimoclomol for inclusion body myositis: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2023;22(10):900-911.
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nat Rev Immunol. 2008 Sep;8(9):726–736.
- Caplan AI, Dennis JE. Mesenchymal stem cells as trophic mediators. J Cell Biochem. 2006 Aug 1;98(5):1076–1084.
- University of Kansas Medical Center. Inclusion body myositis treatment with Celution processed adipose-derived regenerative cells. ClinicalTrials.gov. Identifier: NCT04975841.
- Santos EJF, Farisogullari B, et al. Efficacy and safety of pharmacological treatments in inclusion body myositis: a systematic review and meta-analysis. RMD Open. 2025 Jan 22;11(1):e005176.
- Greenberg SA, Pinkus JL, et al. Highly differentiated cytotoxic T cells in inclusion body myositis. Brain. 2019 Sep 1;142(9):2590–2604.
- Allameen NA, Salam S, et al. Inclusion body myositis and immunosenescence: current evidence and future perspectives. Rheumatology (Oxford). 2025 Mar;64(3):952–961.
- Askanas V, Engel WK, et al. Inclusion body myositis: a degenerative muscle disease associated with intramuscle fiber multiprotein aggregates, proteasome inhibition, endoplasmic reticulum stress and decreased lysosomal degradation. Brain Pathol. 2009 Jul;19(3):493–506.
- Song N, Scholtemeijer M, et al. Mesenchymal stem cell immunomodulation: mechanisms and therapeutic potential. Trends Pharmacol Sci. 2020 Sep;41(9):653–664.
- Tidball JG, Villalta SA. Regulatory interactions between muscle and the immune system during muscle regeneration. Am J Physiol Regul Integr Comp Physiol. 2010 Mar 10;298(5): R1173–R1187.
- Zhang X, Zhang D, et al. Restoration of skeletal muscle function via mesenchymal stem cells: mechanistic insights and therapeutic advances in myasthenia gravis. Front Cell Dev Biol. 2025 Sep 23; 13:1658062.
- Thompson M, Mei SHJ, et al. Cell therapy with intravascular administration of mesenchymal stromal cells continues to appear safe: an updated systematic review and meta-analysis. EClinicalMedicine. 2020 Feb; 19:100249.