A Multidisciplinary Approach in Primary Care: Case Report of Clinical and Social Complexity
Ana Cardoso¹, Alexandra Anjo¹, Carla Novais¹, Mariana Rodrigues¹, Susana Martins2, João Rocha Palas², Tânia Pereira³
DOI: 10.37722/APHCTM.2026105
Watch the Article in Motion
Abstract
Public health challenges frequently arise from the interaction between chronic disease, social vulnerability, and limited access to healthcare. Primary care plays a pivotal role in identifying and addressing these complex needs through integrated, community-based approaches.
We describe the case of a 56-year-old man living in a rural area of Portugal who presented with an infected gluteal ulcer and no prior engagement with healthcare services. Clinical evaluations revealed severe social deprivation, malnutrition, undiagnosed type 2 diabetes mellitus, chronic hepatitis C infection, and suspected autoimmune dermatological disease. Management required coordinated intervention involving primary care physicians, nurses, social workers, internal medicine, hepatology services, and community institutions.
Through a multidisciplinary and community-oriented approach, significant improvements were achieved, including wound healing, glycemic control, nutritional recovery, stabilization of social conditions, and initiation of antiviral treatment for hepatitis C.
This case underscores the importance of integrating public health principles, social care, and clinical management in primary care settings. Addressing social determinants of health through multidisciplinary collaboration in primary care is essential to improve outcomes in socially vulnerable populations and reduce health inequities. Keywords: Public Health; Community Health; Primary Care; Social Determinants of Health; Multidisciplinary Care; Case Report
Introduction
Advances in public and community health emphasize the need to address social determinants of health as fundamental contributors to disease burden and health inequities. Individuals experiencing poverty, social isolation, and inadequate housing often present late to healthcare services, with advanced and overlapping medical conditions.
Primary care is uniquely positioned to serve as the interface between clinical medicine, public health, and community resources. This case was selected because it illustrates a convergence of advanced clinical disease and profound social deprivation encountered in primary care, highlighting the pivotal role of family physicians in identifying hidden vulnerability. Its educational value lies in demonstrating how primary care can act as the first point of contact, care coordinator, and patient advocate, even in the absence of prior healthcare engagement. The case further illustrates how integrated clinical and social interventions can reverse severe health deterioration in a resource-limited, rural context. Case Presentation
A 56-year-old male from Mogadouro, Portugal, presented to the emergency department in September 2023 with a five-day history of pain, edema, and an ulcerated lesion in the right gluteal region (Fig.1).

He had no known chronic illnesses, no regular medication and no previous medical follow-up history. He was an active smoker (17 pack-years) and reported previous alcohol misuse and illicit drug use (cocaine and heroin), discontinued approximately five years earlier.
Physical examination revealed a cachectic, poorly groomed individual with signs of social neglect. Vital signs were stable, and systemic examination was unremarkable except for an infected gluteal ulcer with local inflammatory signs and foul odor. He was treated with antibiotics and wound care and referred to primary care for follow-up.
At the first primary care consultation, marked social vulnerability was identified. The patient lived in a rural and isolated household without electricity, running water, or gas and relied on minimal social income. Family relationships were conflicted, and access to food, medications, and transportation was severely limited.
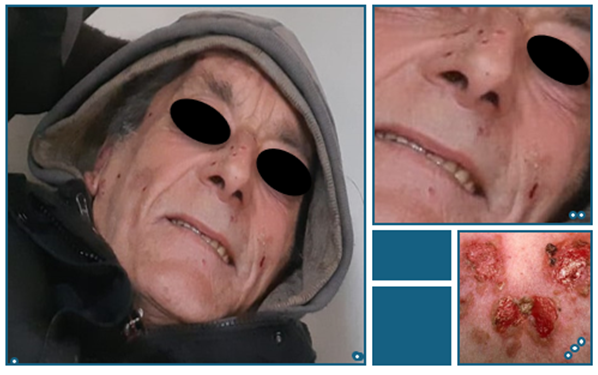
Further assessment revealed significant unintentional weight loss (>20 kg in one year), polyuria, polydipsia, and polyphagia. Laboratory tests demonstrated severe hyperglycemia (fasting glucose >400 mg/dL; HbA1c 15%), elevated liver enzymes, and positive hepatitis C serology with high viral load. Tumor marker CA 19-9 was elevated, prompting extensive investigation. Cutaneous lesions on the face and hands suggested possible pemphigus vulgaris (Fig.2).
Management and Outcomes
Following the initial emergency department visit, the patient was promptly integrated into primary care, where a comprehensive clinical and social assessment was undertaken. In the subsequent weeks, diabetes treatment with basal insulin and oral antidiabetic agents was initiated and progressively titrated, while regular wound care was provided by nursing services (Fig.3), and alcohol abstinence was reinforced.

In parallel, laboratory investigations and imaging studies were conducted. The patient was referred to internal medicine and hepatology for further evaluation. Diagnostic procedures, including endoscopy, colonoscopy, computed tomography, and magnetic resonance imaging, excluded malignant disease. Antiviral therapy for hepatitis C was subsequently initiated.
Social interventions were activated early in the course of care. Social workers and community partners facilitated access to food, hygiene support, transportation, and social services. Primary care maintained close follow-up, ensuring coordination between healthcare professionals and community institutions.
Over the following months of coordinated follow-up, the patient demonstrated substantial clinical and social improvement, including complete wound healing, weight gain, improved hygiene, and better metabolic control, with HbA1c reduced to 8.6%.
Discussion
This case exemplifies how public health challenges manifest at the individual level through the accumulation of social and medical vulnerabilities. The patient’s delayed access to care resulted in advanced disease presentation, while social deprivation significantly hindered self-care and adherence.
Multidisciplinary coordination posed several challenges, including communication across different levels of care, logistical barriers related to rural isolation, and initial difficulties with adherence due to unstable living conditions. These challenges were addressed through structured communication between primary care, nursing, social services, and hospital-based specialists, with primary care assuming a central coordinating role. Establishing trust and adapting interventions to the patient’s social context were essential to ensuring continuity of care.
From a public health perspective, this case reinforces the importance of community-based strategies, early identification of social risk, and multidisciplinary collaboration to reduce health inequities. Although this case occurred in a rural Portuguese setting, the principles underlying the intervention are transferable to other primary care contexts. Early recognition of social determinants, proactive collaboration with community partners, and the positioning of primary care as a coordination hub can be adapted to diverse healthcare systems, including those with limited resources.
Conclusion
Advances in public, community, and primary care health depend on the effective integration of medical and social interventions. This case demonstrates that multidisciplinary, community-oriented primary care can successfully address complex health needs arising from social determinants, leading to meaningful improvements in clinical outcomes and social stability.
Key lessons for primary care practitioners include the importance of recognizing social determinants as central components of clinical complexity, the value of early and sustained multidisciplinary collaboration, and the critical role of primary care as a coordinator across health and social systems. Even in cases of advanced disease and extreme vulnerability, a patient-centered, community-based approach can restore engagement with care and promote long-term health improvement.
Ethics Statement: Written informed consent was obtained from the patient for publication of this case report and associated images. All identifying information was removed to ensure confidentiality and anonymity, in accordance with ethical standards and journal requirements.
Conflict of Interest: The authors declare no conflicts of interest.
References
- Broeiro P. Tangibility of complexity. Portuguese Journal of General and Family Medicine. 2016; 32:87–89. (in Portuguese).
- WONCA Europe. The European Definition of General Practice / Family Medicine. WONCA Europe; 2023.