Percutaneous CT-Guided Aspiration in Pediatric Intracerebral Abscess
Dr. Abass Adam, Dr. Abdul-Aziz Mahama, Dr. Dickson Bandoh,
Dr. Munira Amadu, Dr. Hermas Saamaalme Paaga,
Dr. Okasha Issaka, Dr. Malcolm Mambuoraa Dery*
*Corresponding author: Dr. Malcolm Mambuoraa Dery, Neurosurgery Unit, Department of Surgery, Tamale Teaching Hospital, Tamale, Ghana; Email: malcolmdery135@gmail.com
DOI: 10.37722/JSOTA.2026104
Abstract
Intracerebral abscess is an uncommon but life-threatening intracranial infection. Early diagnosis and prompt intervention are critical to reduce morbidity and mortality, particularly in resource-limited settings.
Case Presentation
We report a 6-year-old male who presented with a two-week history of fever, progressive headache, vomiting, altered mental status, and left-sided weakness. Neuroimaging with contrast-enhanced computed tomography revealed a ring-enhancing lesion in the right thalamus and basal ganglia with surrounding vasogenic edema and mass effect. Magnetic resonance imaging was unavailable due to financial and logistical constraints. The patient was treated with broad-spectrum intravenous antibiotics and underwent computed tomography-guided aspiration, which yielded pus with no bacterial growth on culture. Postoperatively, the child improved significantly, with resolution of fever and neurological deficits. Follow-up imaging at eight weeks confirmed complete resolution of the abscess cavity, and no recurrence was observed after six months.
Conclusion
This case underscores the importance of early recognition, multidisciplinary management, and percutaneous computed tomography-guided aspiration in the treatment of pediatric intracerebral abscess. Even in resource-limited settings, favorable outcomes can be achieved with timely surgical and medical interventions.

Watch the Article in Motion
Keywords
Bentiu, environmental governance, Gas, Oil, Production, South Sudan
Introduction
Intracerebral abscess is a focal intraparenchymal infection of the brain that progresses from cerebritis to a well-formed capsule containing pus. The condition is uncommon but carries significant mortality and morbidity if not recognized and treated early. Intracerebral abscesses commonly arise secondary to contiguous spread from otitis media, sinusitis, dental infections, or hematogenous dissemination from systemic infections. In children, congenital heart disease, immunosuppression, and chronic infections are recognized risk factors.
Advances in neuroimaging, neurosurgical techniques, antimicrobial therapy, and intensive care have significantly improved outcomes. However, delayed diagnosis remains a major contributor to poor neurological outcomes, particularly in low-resource settings where access to advanced imaging modalities such as magnetic resonance imaging (MRI) may be limited.
Pediatric intracerebral abscesses involving deep-seated regions such as the thalamus and basal ganglia are particularly rare and challenging due to their eloquent anatomical location and the associated surgical risks. Previous reports in the literature have demonstrated favorable outcomes with minimally invasive aspiration techniques combined with prolonged antibiotic therapy. Our case further highlights the feasibility and effectiveness of percutaneous CT-guided aspiration in managing deep-seated pediatric brain abscesses in a resource-constrained environment.
Case Presentation
A 6-year-old male presented to the Neurosurgery Unit with a two-week history of progressive headache, fever, vomiting, and altered mental status. The patient subsequently developed left-sided body weakness.
On examination, the child was febrile with a temperature of 38.1 °C and had a Glasgow Coma Scale (GCS) score of 9/15 (E4V1M4). Neurological examination revealed left-sided hemiparesis without obvious cranial nerve deficits. Pupils were equal and reactive to light, and fundoscopy showed no papilledema. Other systemic examinations were unremarkable.
Investigagtion
Baseline laboratory investigations demonstrated leukocytosis with elevated inflammatory markers (WBC: 18 × 10⁹/L; CRP: 15 mg/L). Blood cultures were obtained but showed no bacterial growth.
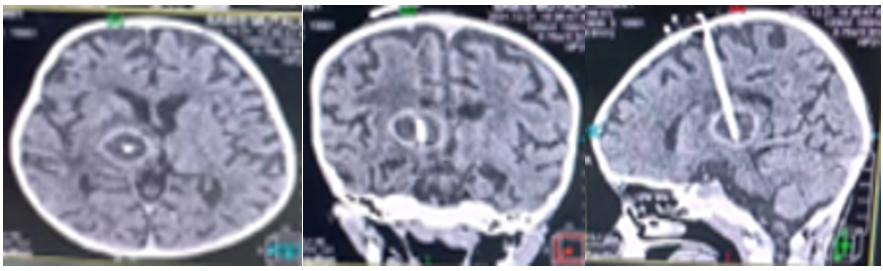
Contrast-enhanced computed tomography (CT) scan of the brain demonstrated a ring-enhancing lesion located within the right thalamus and basal ganglia, associated with surrounding vasogenic edema and mass effect. The imaging findings were highly suggestive of an intracerebral abscess.
Magnetic resonance imaging (MRI) was not performed because of unavailability of MRI services locally and financial constraints limiting travel for further evaluation.
Differential Diagnosis
The differential diagnoses considered included tuberculoma, glioma, fungal abscess and toxoplasmosis. However, the clinical presentation of fever and focal neurological deficits together with the characteristic ring-enhancing lesion and subsequent aspiration of pus supported the diagnosis of pyogenic intracerebral abscess.
Management
The patient was commenced on broad-spectrum intravenous antibiotics consisting of a third-generation cephalosporin and clindamycin. Following multidisciplinary discussions involving the neurosurgery, pediatric, anesthesia, radiology, and critical care teams, the decision was made to proceed with percutaneous CT-guided aspiration because of the deep-seated location of the lesion and associated mass effect.
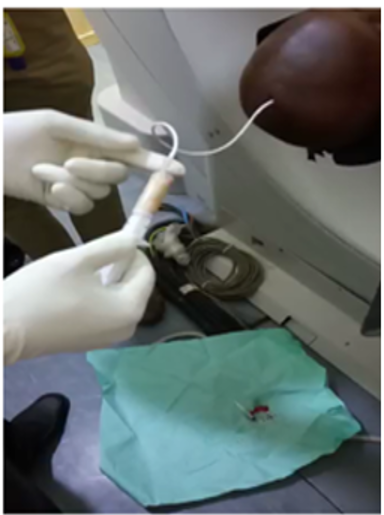
Percutaneous CT-guided aspiration was successfully performed, and purulent material was obtained and sent for microbiological analysis. No bacterial growth was identified on culture, likely secondary to prior antibiotic exposure.
Histopathological evaluation of the aspirated material demonstrated inflammatory cells, necrotic debris, and purulent exudates consistent with pyogenic abscess formation, with no evidence of neoplastic pathology.
Postoperatively, the patient continued intravenous antibiotics with close neurological monitoring.
Outcome and Follow-up
The patient demonstrated gradual neurological improvement following surgery. Fever resolved, mental status improved, and left-sided weakness progressively recovered during hospitalization.
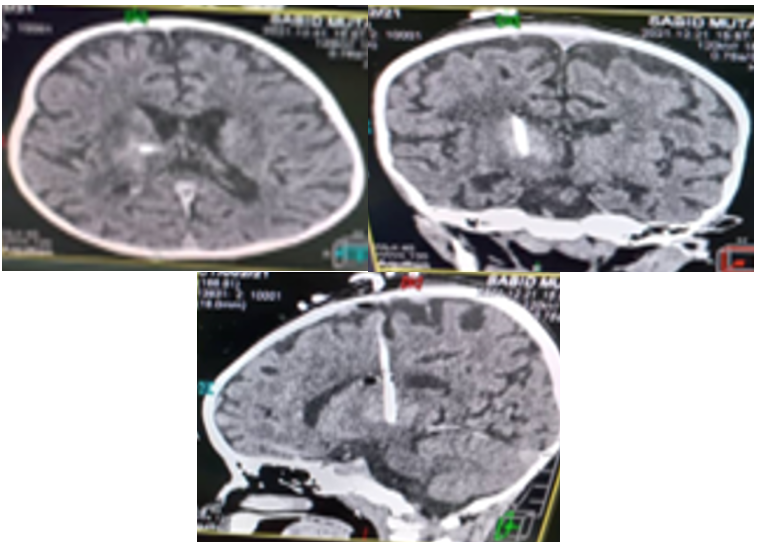
Immediate postoperative CT imaging showed marked reduction in abscess size and surrounding edema. Repeat CT imaging performed eight weeks after aspiration demonstrated complete resolution of the abscess cavity.
The patient was discharged on oral antibiotics and followed up regularly in the neurosurgery clinic. Postoperative monitoring included serial neurological examinations and interval neuroimaging to assess for recurrence or residual infection. No recurrence was observed during six months of follow-up.
Discussion
Clinical Presentation
Intracerebral abscess remains a neurosurgical emergency because of the risk of raised intracranial pressure, cerebral herniation, seizures, and irreversible neurological injury. The classical triad of fever, headache, and focal neurological deficit occurs in fewer than 50% of patients, making diagnosis challenging, especially in pediatric populations. Our patient presented with fever, headache, altered mental status, vomiting, and hemiparesis, which are common manifestations of deep-seated brain abscesses.
Imaging Findinds
Neuroimaging remains central to the diagnosis of intracerebral abscess. Contrast-enhanced CT scanning typically demonstrates a ring-enhancing lesion with surrounding edema and mass effect, while MRI offers superior characterization and diffusion-weighted imaging sensitivity. In our patient, CT imaging demonstrated a characteristic ring-enhancing lesion in the right thalamus and basal ganglia. Although MRI was unavailable, CT findings combined with clinical presentation were sufficient to guide urgent management.
Previous pediatric reports of deep-seated intracerebral abscesses have similarly emphasized the utility of CT imaging and stereotactic or image-guided aspiration in settings where MRI access is limited.
Surgical Management
Management of intracerebral abscesses generally includes a combination of antimicrobial therapy and surgical intervention. Deep-seated abscesses located within eloquent structures such as the basal ganglia and thalamus pose significant surgical challenges. CT-guided aspiration provides a minimally invasive and effective therapeutic option that reduces intracranial pressure, allows microbiological diagnosis, and minimizes injury to surrounding brain tissue.
In our patient, percutaneous CT-guided aspiration resulted in rapid clinical improvement and radiological resolution. The absence of bacterial growth on culture has been reported in prior studies and may be related to preoperative antibiotic administration.
Multidisciplinary management involving neurosurgeons, pediatricians, radiologists, microbiologists, anesthetists, infectious disease specialists, and critical care teams remain essential for optimizing outcomes in pediatric intracerebral abscesses.
Prognosis and Recurrence Risk
The prognosis of intracerebral abscess depends largely on early diagnosis, prompt initiation of antibiotics, neurological status at presentation, and adequacy of surgical drainage. Advances in imaging and minimally invasive neurosurgical techniques have significantly improved survival rates.
Recurrence risk is generally associated with incomplete drainage, persistent infective focus, immunosuppression, or inadequate antibiotic therapy. Careful postoperative monitoring with serial neurological assessment and follow-up imaging is therefore important. In our case, no recurrence was observed after six months of follow-up, indicating favorable treatment response.
Conclusion
Intracerebral abscess is a life-threatening but treatable neurosurgical condition. Early recognition, appropriate neuroimaging, timely surgical intervention, and prolonged antimicrobial therapy are essential for favorable outcomes.
This case demonstrates that CT-guided aspiration remains an effective and practical management strategy for deep-seated pediatric intracerebral abscesses, particularly in resource-limited settings. Furthermore, multidisciplinary collaboration and structured postoperative follow-up are critical components in minimizing morbidity and recurrence.
Reference
- Brouwer MC, Tunkel AR, McKhann GM, van de Beek D. Brain abscess. New England Journal of Medicine. 2014;371(5):447–456. https://doi.org/10.1056/NEJMra1301635
- Mathisen GE, Johnson JP. Brain abscess. Clinical Infectious Diseases. 1997;25(4):763–779. https://doi.org/10.1086/515541
- Moosa ANV, Rajshekhar V. Management of brain abscess: An overview. Neurosurgical Focus. 2008;24(6):E3. https://doi.org/10.3171/FOC/2008/24/6/E3
- Helweg-Larsen J, Astradsson A, Richhall H, Erdal J, Laursen A, Brennum J. Pyogenic brain abscess, a 15-year survey. BMC Infectious Diseases. 2012; 12:332. https://doi.org/10.1186/1471-2334-12-332