Changes And Perception of Social Roles in People After Acquired Brain Injury (ABI)
Simona Tičar*, Mateja Korošec, Eva Ristič
DOI: 10.37722/APHCTM.2026102
Social roles – such as partner, parent, friend, worker and active member of the community – are central to an individual’s social identity and contribute significantly to their sense of personal worth, belonging and meaning. After ABI, these roles often change significantly or the individual can no longer identify with them in the same way as before the injury.
As a result, a process of so-called identity reconstruction can develop, which is often marked by feelings of loss of the former self, reduced self-esteem and social marginalization.
Despite the growing interest in the psychosocial aspects of rehabilitation of people with ABI, most research still focuses on individual symptoms (e.g. depression, anxiety, social isolation). A comprehensive analysis of changes in social roles and their subjective experience is crucial for understanding the long-term challenges that injured people and their relatives face in everyday life, and for developing effective support and rehabilitation interventions.
The purpose of this work is therefore to examine in depth the changes and perception of social roles of persons after acquired brain injury and to shed light on their impact on identity, the quality of interpersonal relationships and the level of social inclusion. Special attention is also paid to the role of the family and social environment in the process of adaptation and the formation of new patterns of functioning after injury.

Watch the Article in Motion
In this way, the research contributes to the understanding of PMP as not only a medical, but also a comprehensive rehabilitation challenge, which emphasizes the need for comprehensive rehabilitation approaches, which also include support in the re-establishment of social roles, relationships and a sense of personal continuity.
The consequences of acquired brain injury (ABI) are numerous and manifest across all domains of human functioning: physiological, physical, emotional, cognitive, and behavioral (Vešligaj Damiš & Korošec, 2019). Individuals with ABI often experience difficulties in social functioning, such as how they act and behave in various social situations, interpersonal relationships, and within society at large. These difficulties may persist long after the injury or even become permanent.
The consequences of ABI affect the individual’s activities and social participation throughout various stages of life after the brain injury. Due to the effects of ABI, individuals may face extensive long-term limitations in their abilities, which impact:
- independent living,
- mobility – including the ability to drive or use public transportation,
- return to work or education,
- participation in leisure, sports, and social activities,
- fulfillment of family roles,
- management of personal, sexual, and family relationships, and
- engagement in other life activities (Vešligaj Damiš & Korošec, 2019).
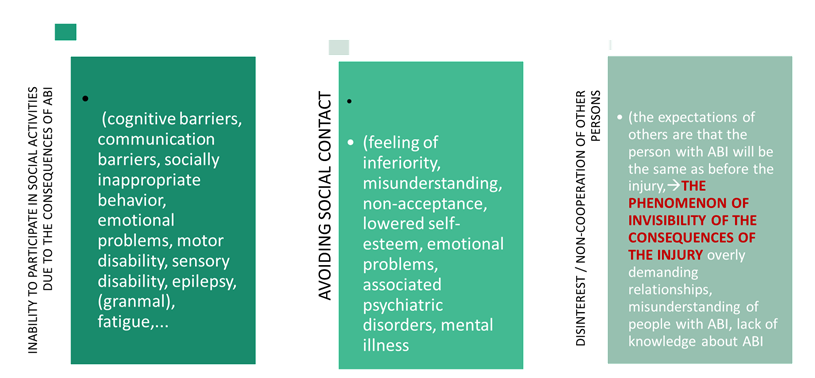
After an acquired brain injury (ABI), relationships with friends often change significantly. Friends may not fully understand the nature of the changes and frequently hope or expect that the person will return to being “the same” as they were before the injury. Due to a general lack of awareness about the consequences of brain injury, friends often misinterpret the survivor’s altered behavior. As a result, relationships may gradually weaken, and many friendships end altogether. Consequently, individuals with ABI often feel misunderstood and unaccepted, which can lead them to withdraw from social interactions, resulting in social isolation and loneliness (Vešligaj Damiš & Korošec, 2019).
In the early stages following the injury, friends may offer support, express affection, and provide encouragement. Over time, however, it becomes important for the individual with ABI to re-establish, strengthen, and appropriately reshape interpersonal relationships. ABI may alter a person’s social network: some former acquaintances and friends may discontinue contact, while new connections may be formed (Radonjić Miholić, 2009).
Even five years after the injury, family members or other close individuals often report ongoing difficulties in the ABI survivor’s social functioning, personality, and behavior (Hillier & Metzer, 1997).
At the same time, family members of individuals with ABI frequently report the loss of previous friendships, as they are no longer able to participate in shared activities as they did before the injury—often due to reduced physical abilities or cognitive, behavioral, and/or personality changes. Family members themselves commonly feel misunderstood by others and experience inadequate responses from their social environment, which may result in the social isolation of the entire family.
Individuals with brain injuries also tend to participate less in organized social events and community life, as they are often hindered by cognitive, physical, emotional, and social difficulties.
Family
An acquired brain injury (ABI) often leads to significant changes in the dynamics of the family system. An individual who previously functioned as a caregiver, parent, or primary income provider may become dependent on others for support. These shifts frequently cause emotional distress, interpersonal conflict, and necessitate a restructuring of family relationships (Kreutzer et al., 2009). Family members—especially partners—are often forced to take on new caregiving roles, which can lead to emotional exhaustion and strain on the couple’s relationship.
According to Boss and Couden (2002, in Segev, 2018), the lack of clarity about the injured person’s condition makes it difficult for the family to cope with the situation and prevents them from engaging in the grieving process. This ambiguity can lead to decision-making difficulties, depression, anxiety, loss of control, a sense of helplessness, and unclear boundaries within family relationships.
The ability to build and maintain relationships requires communication skills, cognitive functioning, and physical capabilities—all of which may be impaired after ABI. In working with individuals with ABI, clinicians frequently observe challenges such as difficulty perceiving others’ emotions, a lack of empathy, inappropriate emotional responses in various situations, socially unacceptable behaviors, and failure to observe normative behavioral expectations in the home or in public. Egocentricity or the prioritization of one’s own needs regardless of the context or others is also common. These impairments significantly affect the development of social networks, the quality of interpersonal relationships, and the individual’s self-image (Douglas, 2019; Vešligaj Damiš & Korošec, 2019).
According to Roberts (2014, in Segev, 2018), conflicts and disputes within the family may lead to emotional alienation—both from oneself and from other family members. These tensions disrupt communication and hinder the recognition of each other’s needs.
Brain injury often disrupts traditional family roles. It is essential that family responsibilities and roles are thoughtfully reallocated post-injury to prevent some members from becoming overwhelmed. Every family has its own mechanisms for coping with difficulties while striving to maintain its core roles and functions. However, family members caring for an individual with ABI may neglect their own needs, which can lead to exhaustion, feelings of helplessness, depression, and various physical or mental health problems (Radonjić Miholić, 2009).
Families caring for individuals with ABI also frequently face financial challenges and an increasing burden of additional social roles. Social isolation is a common consequence, affecting overall family functioning. If the injured person was the main income earner, the financial stability of the family may be at risk. Household income often decreases when other family members are unable to find additional sources of income. Research has shown that caregivers with limited support are at higher risk for physical and mental health strain (Azman et al., 2020).
Following ABI, social roles within the family are often redistributed, disrupting the family’s internal balance (Whiffin et al., 2021). One major shift is the transition of a partner into the role of caregiver. Family members are required to adapt to a new daily rhythm and actively reassign roles and responsibilities within the family unit.
Family members are often required to assume new roles or experience role reversals (e.g., a child taking on the care of a parent), as individuals with acquired brain injury (ABI) frequently can no longer fulfill their previous roles within the family and society. In an American study involving adults with ABI (Hallet, 1994, as cited in Vešligaj Damiš & Korošec, 2019), every participant reported a change in at least one of their former social roles, and 64% reported the loss of three or four roles.
A key element of family life is the sense of belonging, shared purpose, and the presence of a supportive social network. Research shows that families gradually adjust to altered social roles over a period of up to seven years post-injury. Families shared diverse experiences in their journey toward achieving stability. A common theme among all families, however, was the struggle with loneliness. This included self-imposed isolation, as individuals with ABI often withdrew from social situations and declined invitations to gatherings. Caregiving family members frequently reported feeling alone, with no one to share their burden or provide relief (Stenberg, Stålnacke, & Saveman, 2024).
Research by Sander (2002) highlights that family functioning is a crucial variable to be included in future predictive models of rehabilitation outcomes. Moreover, family-based interventions should be recognized as an essential part of the rehabilitation process.
As emphasized by Vešligaj Damiš & Korošec (2019), family members must take on new responsibilities or exchange roles within the family system, as individuals with ABI often lack the capacity to continue performing their previous roles in the household and the broader community.
Partnerships
Partnerships often become imbalanced following an acquired brain injury (ABI), as one partner typically assumes the role of caregiver. Changes in sexuality, emotional closeness, and the sense of partnership are common and require adjustment on both sides.
ABI frequently leads to significant changes in romantic relationships and sexual functioning. Research suggests that men are more likely to conceal deficits in sexual and relational competence due to ego-related concerns and societal role expectations (Tičar & Ristič, 2022).
Deficits related to ABI can destabilize the core of a partnership by impacting roles, responsibilities, trust, communication, emotional connection, and mutual behavior (Hammond et al., 2011). ABI may directly affect sexual functioning or indirectly impair motor, sensory, cognitive, behavioral, and emotional capacities (Oddy, 2001). These changes in individuals with ABI also appear to influence the sexuality of their uninjured partners (Downing & Ponsford, 2018).
Spouses often take on extensive responsibilities for the injured partner, even though they may have little or no prior experience with caregiving. Some spouses have reported sentiments such as, “I am married, but I have no husband,” or “I’m married to a stranger” (Kreutzer, Godwin, & Marwitz, 2010).
Individuals with ABI may struggle with the realization of how their partner feels, which can lead to perceptions that their partner is now with a “different person” or a “stranger.” This can result in a shift in relationship roles, often described as a disruption in the partnership, and feelings of having lost the person they originally fell in love with. A recent review found that impairments in social cognition in the injured partner can negatively affect relationship satisfaction as reported by the uninjured partner (Falshaw et al., 2024).
Family members frequently report problems such as social isolation, altered family roles, depression, anxiety, and more frequent physical health issues (Kolakowsky-Hayner, Miner & Kreutzer, 2001, as cited in Vešligaj, 2019).
Following ABI, the injured individual may lose employment and spend more time at home, with diminished capacity to fulfill roles as a parent, grandparent, or caregiver to aging parents. The healthy partner takes on additional responsibilities, eroding reciprocity and equality in the relationship and often giving rise to conflict (Northcott et al., 2015, as cited in Maglica, 2023).
Anxiety
After a stroke, anxiety often arises due to the individual’s inability to return to their previous level of functioning and the perceived discrepancy between who they currently are and who they believe they should be (as cited in Sešok et al., 2015). Feelings of helplessness and dissatisfaction with everyday functioning may lead individuals with acquired brain injury (ABI) to withdraw from social interactions. Anxiety can also indirectly prolong the recovery process, particularly in re-learning everyday tasks (Sešok, 2015).
Anxiety is commonly a byproduct of the psychological adjustment to life after injury. It results from a loss of perceived control and from uncertainty regarding the future and one’s social role (Vešligaj Damiš & Korošec, 2019).
Another study (Viscogliosi, Belleville & Desrosiers, 2011, as cited in Sešok, 2015) found that older adults who had suffered a stroke were generally more successful in performing routine daily tasks six months post-injury. However, they tended to abandon social roles they perceived as too demanding. For example, due to deficits in language and executive functioning, they often avoided socializing with friends because they struggled to find appropriate words and exhibited slowed speech and response times. These behaviors were also influenced by motivational and emotional deficits.
Unlike essential daily tasks, social activities are more reliant on personal desires, interests, and intrinsic motivation. Therefore, social engagement is considered a higher-order need—some even place it within the realm of self-actualization—which demands significant compensation for existing deficits (Viscogliosi, Belleville & Desrosiers, 2011, as cited in Sešok, 2015).
If a person with ABI experiences difficulties with self-initiation, this typically affects both their ability to carry out daily activities and their capacity for social participation (e.g., managing errands at the bank or grocery shopping).
Functioning in the Environment
Social isolation is a common consequence of acquired brain injury (ABI) and is often considered one of the most profound life changes for individuals with traumatic brain injury (TBI). It has a significant negative impact on the quality of life. Contributing factors include reduced initiative, communication disorders, emotional instability, and societal stigma.
Social isolation refers to a decrease in both the quantity and quality of interpersonal relationships across various levels of interaction—individual, group, community, and broader society (Zavaleta et al., 2014, as cited in Salas et al., 2021). Two key factors in studying social isolation are the number of social relationships and their quality.
Effective integration of individuals with ABI into their immediate and broader environments requires that both they and their families are well-informed about the injury and its consequences. Individuals with ABI should be encouraged to resume their previous life roles and participate in leisure activities to the extent possible and within their functional abilities. Participation in such activities is closely linked to health status and overall quality of life and can serve as a strong starting point for rebuilding an active lifestyle. In some cases, new social roles and leisure pursuits must be identified that are tailored to the person’s functional capacity.
The restoration of driving ability also increases opportunities for successful reintegration and reduces isolation. More than half of stroke survivors cease driving (Goljar, n.d.), and the inability to drive can provoke intense emotional responses, such as a sense of loss, social inequality, and personal devaluation, despite the reality that certain abilities are essential for safe driving (Kuralt , Goljar, 2009).
In older adults post-stroke, reduced ability to perform extended daily tasks (e.g., cooking, laundry, shopping) negatively affects their sense of life control and reduces opportunities for personal growth and positive social interaction (Kuralt, Goljar, 2009).
Through the integration of structured leisure activities into rehabilitation, social contact and social roles can be expanded, supporting quality free-time engagement, personal growth, and reintegration into the broader social environment (Vešligaj Damiš, Korošec, 2019).
Emotional and behavioral changes following ABI are numerous and may include emotional lability, agitation, aggression, impulsivity, irritability, and more passive symptoms such as depression and apathy (Braine, 2011).
ABI has been shown to have a profound, long-term, and negative impact not only on the individual’s everyday life but also on the lives of their family members (Jumisko, Lexell & Söderberg, 2007; Testa et al., 2006, as cited in Braine, 2011).
While individuals in early or middle adulthood are typically active in education, employment, or other pursuits, rehabilitation after ABI is often a complex and demanding process. Possible outcomes of rehabilitation include returning to work or school, job adaptation, employment in a sheltered workplace, or retirement. Sometimes, individuals may secure employment during rehabilitation but later find themselves unable to meet the demands of their role. In such cases, if resources allow, they may re-enter long-term, comprehensive rehabilitation. At the Center Korak in Kranj, Slovenia, users may continue to receive support even after completing the formal rehabilitation program.
Researchers have documented a long-term decline in both the number and depth of social relationships after ABI. This social isolation reflects a reduced ability to maintain pre-injury marital and friendship ties and difficulty forming new social connections. Many individuals with ABI experience increasing isolation and may develop various mental health conditions, often failing to achieve optimal psychosocial functioning due to a lack of necessary support. It is crucial to help individuals develop meaningful social roles within their communities (Haslam et al., 2008).
People with TBI often report a reduction in their social networks and a loss of friendships formed before the injury, as well as a decrease in perceived social support, fewer opportunities to establish new friendships, and limited involvement in leisure activities—factors that contribute to high levels of social isolation (Bier, Dutil & Couture, 2009).
Emotional Recognition, Empathy, and Social Impact of ABI
Individuals with acquired brain injury (ABI) consistently report difficulties in recognizing emotions in facial expressions and vocal tones, although not all experience impairments in both modalities. Empathy plays a crucial role in successful interpersonal relationships by enabling individuals to understand and respond to the emotional experiences of others (Decety & Jackson, 2004).
In recent years, interest in emotional empathy has increased, particularly in relation to the concept of emotional contagion, which is defined as the “tendency to mimic the verbal, physiological, and/or behavioral components of another person’s emotional experience/expression and thereby come to feel/express the same emotions oneself” (Hsee, Hatfield, Carlson, & Chemtob, 1990, p. 328, as cited in Sousa et al., 2012).
Neuropsychological studies have often focused on cognitive empathy (Roger et al., 2008). Cicerone et al. (1983) found that the ability to respond empathetically was linked to cognitive flexibility. Pessoa argues that it is not possible to separate the cognitive and emotional contributions of the brain to executive control; emotion and cognition interact and contribute equally to the regulation of thought and behavior.
Social Isolation and Loneliness
Social isolation (i.e., the objective lack of social contact or connection) is distinct from loneliness (i.e., the subjective perception of being alone or lacking desired social interaction) (Heinrich & Gullone, 2006). Individuals with ABI report higher levels of loneliness as well as smaller and more limited social networks (Morton, Wehman, 1995).
Rehabilitation professionals have increasingly recognized the importance of social interaction in the reconstruction of identity. According to social identity theory, group membership and the development of social identities are fundamental therapeutic components in modern rehabilitation models (e.g., Haslam et al., 2012, 2018; Salas et al., 2020). These approaches emphasize the role of social connectedness in supporting recovery, well-being, and a sense of self.
Social Consequences of Stroke
The social consequences of stroke are profound. Stroke survivors tend to engage in fewer activities, experience disruptions in family life, and suffer from weakened social ties with friends and their broader networks. Studies have shown that, following ABI, contact with friends and participation in social activities decrease. However, the perceived emotional support from family members tends to remain stable (Northcott et al., 2015).
These findings underscore the importance of addressing emotional and social dimensions in the rehabilitation of individuals with ABI, particularly through interventions aimed at enhancing empathy, rebuilding social networks, and fostering meaningful social roles and group membership.
Identity changes
One of the most common consequences of TBI is the loss or change of employment role. Due to cognitive, physical and behavioural changes, many individuals are no longer able to perform their profession after brain injury. This often leads to reduced self-esteem, feelings of loss of meaning and social isolation (Ownsworth & Haslam, 2006).
Work not only provides an individual with financial security, but also an important source of self-affirmation and social identity. One of the most deeply experienced effects of TBI is an identity crisis, which results from the sudden loss of previously formed social roles. Nochi (1998) describes this phenomenon as a “loss of self”, where individuals express the feeling that they are “no longer who they used to be”. Changes in abilities, behaviour and social role can lead to a breakdown of the previous sense of self, which is associated with depression, feelings of inferiority and a loss of meaning in life.
Method
Participants
Two groups were included in the study: an experimental group (people with acquired brain injury, PMP) and a control group (people without brain injury). All participants voluntarily gave written consent to participate, and anonymity was guaranteed.
The experimental group consisted of 33 adults with ABI (21 men, 12 women), included in the comprehensive rehabilitation program of the Center Korak Kranj. Participants were selected based on their ability to communicate and expressed interest in participating. They completed five questionnaires that measured interpersonal relationships, socio-psychological well-being and functioning; not all participants completed all questionnaires due to individual limitations. 17 participants completed the entire battery.
The average time from the onset of brain injury to the execution of the study was 10 years.
The control group consisted of 30 participants (10 men, 20 women), all in a partner relationship, who completed the entire battery of five questionnaires. The control group was formed using the snowball method.
The data were analyzed using Excel and the statistical program SPSS.
Instruments
ECR-R
The Experiences in Close Relationships – Revised questionnaire (ECR-R; Fraley, Waller, & Brennan, 2000) is a self-report instrument consisting of 36 items that assess attachment in adult romantic relationships, evaluating attachment within specific relationship contexts. ECR-R is a revised version of the original ECR questionnaire (Brennan, Clark, & Shaver, 1998). The Slovenian version was translated and adapted by Sraka (2007). Both questionnaires measure individual differences in attachment along two dimensions, each comprising 18 items rated on a 7-point Likert scale (1 – not at all characteristic of me, to 7 – very characteristic of me).
- The anxious attachment dimension evaluates fear of abandonment and rejection
- The avoidant attachment dimension evaluates discomfort with closeness
Final scores are calculated as the mean of item responses within each dimension. - Social Support Questionnaire – SSQ6 (Sarason et al., 1987)
The SSQ6 is the Slovenian version of the Social Support Questionnaire – Short Form (translated by Tanja Lamovec, 1988). It consists of two parts, each with six items: - SSQ-N assesses the perceived number of social supporters.
- SSQ-S assesses satisfaction with perceived social support.
- Participants list up to nine individuals who support, accept, help, or uplift them. They then rate their average satisfaction with the support for each item on a scale from 1 (very satisfied) to 6 (very dissatisfied). Sarason et al. (1987) reported high reliability coefficients across three samples (α = .90–.93) for both support quantity and satisfaction.
- The SSQ6 provides key insights into:
- the number of individuals participants consider significant in their lives,
- the structure of their social network (e.g., faily, friends, professionals),
- satisfaction with perceived social support.
- (HIFDS – How I Feel in Different Situations, Bonino, Lo Coco, & Tani, 1998)
The HIFDS consists of 12 items designed to assess two dimensions of empathy: - Cognitive empathy (6 items)
- Affective empathy (6 items)
Responses are given on a 4-point Likert scale ranging from 0 (never true) to 3 (always true).
Each subscale (cognitive and affective empathy) yields a total score ranging from 0 to 18, with higher scores indicating greater empathic capacity in the respective domain.
UCLA Loneliness Scale (Russell, Peplau & Curtona, 1980; Russell, 1996)
The Slovenian version of the UCLA Loneliness Scale contains 20 items (e.g., “How often do you feel that you are not close to anyone?”), with participants rating the frequency of these experiences on a 4-point scale (1 – never, 2 – rarely, 3 – sometimes, 4 – always).
Half of the items are reverse-scored (indicating non-loneliness) to ensure validity.
Multidimensional Relationship Questionnaire (MRQ)
Developed by Snell, W. E., Jr., Schicke, M., & Arbeiter, T., the MRQ explores various characteristics of an individual’s romantic relationship across 12 subscales:
- Relationship Esteem
- Relationship Preoccupation
- Internal Relationship Control
- Relationship Consciousness
- Relationship Motivation
- Relationship Anxiety
- Relationship Assertiveness
- Relationship Depression
- External Relationship Control
- Relationship Monitoring (concern about others’ opinions)
- Fear of Relationship
- Relationship Satisfaction
Each subscale provides a multidimensional insight into the psychological and emotional aspects of romantic relationships.
Results With Interpretation
Table: Overview of differences between the PMP and KS groups by dimensions and questionnaires.
| Questionnaires | GROUP | N | M | SD | SE | Statistical test result |
| HIFDS Cognitive empathy | ABI | 31 | 13,65 | 2,775 | ,498 | U=328,00 z=-1,993 p= ,046 |
| HIFDS Cognitive empathy | ABI | 30 | 14,63 | 3,000 | ,548 | |
| HIFDS Affective empathy | CG | 31 | 16,35 | 3,791 | ,681 | U=428,00 z=-1,993 p= ,597 |
| HIFDS Affective empathy | CG | 30 | 16,60 | 3,701 | ,676 | |
| SSQN | ABI | 28 | 2,8282 | 1,74157 | ,32913 | U=181,00 z= -3,722 p= < ,001* |
| CG | 30 | 4,4470 | 1,80053 | ,32873 | ||
| SSQZ | ABI | 28 | 5,4725 | ,60421 | ,11418 | U=375,50 z= -,724 p= ,469 |
| CG | 30 | 5,4943 | ,95955 | ,17519 | ||
| UCLA | ABI | 29 | 40,83 | 10,37 | 1,901 | U=285,50 z= – 2,271 p= ,023 |
| CG | 30 | 35,13 | 3,141 | 1,121 | ||
| ECR-R (Avoidance) | ABI | 18 | 2,6852 | 1,082 | ,256 | U=160,00 z= – 2,34 p= ,019 |
| CG | 30 | 2,0222 | ,678 | ,124 | ||
| ECR-R Anxiety | ABI | 18 | 4,6871 | ,510 | ,120 | U= 1,00 z= -5,73 p= < ,001* |
| CG | 30 | 1,9685 | ,668 | ,122 | ||
| ECR-R MOTHER | ABI | 17 | 3,8926 | 1,068 | ,260 | U=134,50 z= – 2,153 p= ,031 |
| CG | 26 | 3,2615 | ,521 | ,102 | ||
| ECR-R FATHER | ABI | 15 | 3,4917 | ,975 | ,251 | U=163,00 z= – 1,040 p= ,298 |
| CG | 27 | 3,3037 | ,432 | ,083 |
Significant differences were found between the ABI and CG groups in several psychological domains. The PMP group has higher levels of loneliness, higher levels of anxiety and avoidance in interpersonal relationships, and stronger insecure attachment patterns, especially about attachment to the mother. There were also differences in cognitive aspects, where the KS group achieved higher results, while emotional states were similar between the two groups. These results indicate differences in psychological and social functioning between the two groups.
From the SSQN questionnaire, which is intended to measure social support, we obtained three more key pieces of information:
-the number of people that participants report as important in their lives,
-insight into the structure of the social network (family, friends, professionals, etc.) from which participants receive support in everyday life, and
-satisfaction with perceived social support.
One person in CG listed 5 friends as social support. CG has a large social circle of social support, which is not limited to family members, friends stand out, they listed as many as 57. ES (ABI) list close and closest family members as social support, one person also lists a dog as support. Some individuals in EG (ABI) perceive the Center KORAK, Kranj and the professional workers employed at the KORAK Center, Kranj, as social support, as they are involved in the process of long-term and comprehensive rehabilitation after ABI.
People after ABI reported a smaller social network compared to the control group.
Table: Comparison of groups by reports of social support.
| ES -PMP | KS |
| Perception of social support is low. | Perception of social support is higher. |
| The number of support persons is small – family members predominate (0-10) | The number of support people is high – on average it extends to a larger number of friends, they also rely on their own parents |
| A good half of participants are in a relationship, and more of them also describe an imaginary relationship. | Multidimensional relationships – the more people evaluate the current relationship, the more people are in the relationship |
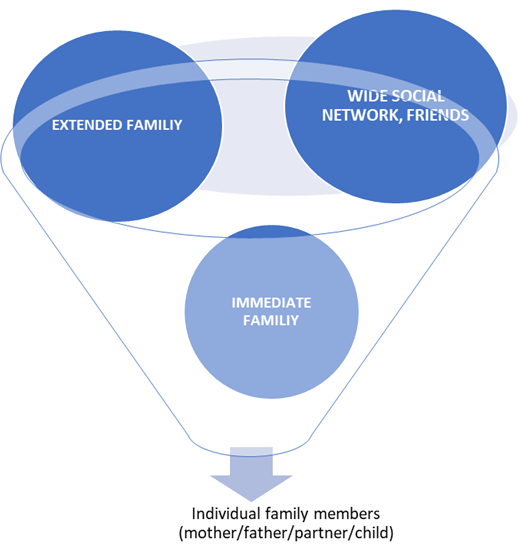
The results show that over a certain period, the social network shrinks. People with ABI first lose social contacts or social support in the wider social network (friends, colleagues, neighbours, etc.). Then the social network shrinks according to the funnel principle, where people with ABI also lose social support in the wider family and narrow down to members of the immediate family, where only certain family members remain (mother, father, child, partner, etc.), only one family member can remain as support.
The process of shrinking the social network begins a few months after ABI and crystallizes within 2-3 years after the injury. The length of the process depends on several factors: the previous social network of the individual with ABI, the complexity of the injury, the individual’s personality… The causes of shrinking the social network are speech impediments, fatigue, physical obstacles (revocation of driving license, immobility), lack of motivation, mutual over-demandingness in interactions, …
More opportunities to maintain social contacts or People with ABI who are in a partnership have social networks (family friends, friends of the partner, new friends, etc.). People without a partner have reduced opportunities to maintain existing social contacts and build a new social network. People after ABI who are involved in the process of long-term and comprehensive rehabilitation have more opportunities and possibilities to establish interpersonal relationships that they feel as social support (employees, volunteers, co-users, etc.). It has been proven that the process of long-term rehabilitation affects the quality of life of people with ABI.
Why reduced social contacts?
Hypothesis 1:
Regardless of the social support they feel they have; EG and CG participants are satisfied. Social isolation is the most profound change for people with ABI – after an injury, social support narrows from a wide network of friends to the closest family members. There are almost no friends left. People with ABI were similarly satisfied with social support as the control group, which is not consistent with the results of Tomberg et al. (2005, in Maglica 2023), as their participants were less satisfied with the support they received compared to the general population.
Experience Of Relationships with Close People (Ecr-R)
Hypothesis 2:
- Is there a connection between experiencing anxiety in relationships (MRQ) and anxiety in relationships with close people (ECR-R)?
In CG, there is a negative correlation between anxiety in relationships (MRQ) and anxiety in relationships with close people (ECR-R); therefore, anxiety in relationships can arise from social relationships, which means that the person does not transfer anxiety to a partner or other relationship.
In EG, anxiety in social relationships does not arise from the relationships themselves, but people with EG look for causes within themselves (I am not good enough, communication problems, …). In the control group, anxiety in relationships arises from the relationship itself (perception of the relationship causes anxiety).
- Does avoidance in relationships correlate (ECR-R) with social support (SSQN)?
The results show a negative correlation between avoidance in relationships and perceived social support in both groups:
• in the EG group: r = –0.509*, p < 0.005
• in the CG group: r = –0.512**, p < 0.001
EG and CG individuals who avoid relationships consequently also have a reduced number of people who provide them with social support. People with ABI are on average reluctant to show their deepest emotions to their partner, and they also have difficulty allowing themselves to be dependent on their partner, so in the case of very intimate situations and dilemmas they do not have or cannot receive support from family members, partners, etc.
- Does an individual transfer social anxiety from partner relationships to all social relationships?
In people with ABI, anxiety can be perceived as a consequence of ABI. Anxiety in relationships, when people, for example, worry about whether they are competent to their partner, is not transferred or generalized to other relationships. The questions of whether an individual is good enough or will be able to do it are influenced by low self-esteem and coping with changes after ABI.
In the clinical group (CG), a statistically significant negative correlation was found between the dimension of attachment anxiety and the size of the social network (r = –0.495**, p < 0.001). In contrast, in the experimental group (EG), this connection was not statistically significant (r = –0.083), which indicates the absence of a connection between the two variables in this population.
Results in the clinical group suggest that higher levels of anxious attachment, characterized by intense fear of rejection, doubts about one’s own worth within relationships, and an excessive need for validation, coincide with a smaller number of people on whom one can rely for social support. Individuals with high relationship anxiety often doubt their own ability to establish and maintain stable, intimate relationships.
Fears of abandonment, uncertainty about a partner’s emotional availability, and hypersensitivity to signs of rejection may also contribute to withdrawal or passivity in establishing broader supportive bonds. As a result, these individuals’ social networks may shrink or remain limited over time. The lack of such connectedness in the ES group may indicate heterogeneity of attachment experiences in this group or the presence of other moderating factors that mitigate the impact of anxious attachment on perceived social network size.
Anxiety in social relationships by persons with ABI does not arise from the relationships themselves, but rather people look for the causes of anxiety within themselves
(I’m not good enough, communication problems,).
In the control group, anxiety in relationships stems from the relationship itself (perception of the relationship causes anxiety).
Stronger anxiety in the partner relationship (ECR-R) is statistically significantly reported by individuals after ABI compared to CG.
They often worry that their partner will leave them.
It is difficult to accept that they would be dependent on their partner.
In individuals with PMP, the social network does not decrease due to fear in the relationship and the reasons for this lie elsewhere.
Although individuals with PMP often express a higher level of anxiety in partner relationships (measured with the ECR-R scale) compared to individuals in the control group (CS), this does not affect the number of significant others in their social network. The statistically significant difference between the two groups indicates that individuals with PMP often worry about being abandoned by their partner, and at the same time find it difficult to accept emotional dependence on their partner.
Interestingly, no statistically significant differences were found between the two groups in the perception of support from parents (mother and father). Participants in both groups report that they can rely on their parents in case of distress (or have relied on them in the past, if their parents are no longer alive). Parents provide them with emotional support and are often people with whom they can openly discuss their problems.
Furthermore, the analysis did not show statistically significant differences between the groups in terms of perceived cognitive and emotional empathy. Although individuals with PMP on average reported slightly lower levels of both dimensions of empathy, they nevertheless showed a similar ability to understand and experience the emotions of others as individuals from the control group.
In the control group (CG), a high and statistically significant positive correlation was found between perceived support from mother and father (r = 0.718**, p < 0.001), indicating that individuals from the general population were able to rely on both parents to the same extent and talk to them about their problems.
Psychosocial Aspects of Relationships in Individuals with Acquired Brain Injury
A comparison between the experimental group (EG) and the group of individuals with acquired brain injury (ABI) did not show statistically significant differences in dimensions related to the experience and evaluation of partner relationships. Specifically, differences were not present in the areas of self-evaluation in the relationship, preoccupation with the relationship, internal and external locus of control, awareness of the relationship, desire for the relationship, anxiety in the relationship, fear of the relationship, and general satisfaction in the relationship. These data indicate that individuals with ABI do not differ significantly from the general population in many key psychological aspects of experiencing partner relationships.
Nevertheless, significant differences were found between the two groups on three dimensions that have important implications for psychosocial rehabilitation. Individuals with PMP reported:
• statistically significantly lower assertiveness in relationships (M = 19,53; SD = 3,026), which may indicate a reduced ability to clearly express one’s own needs, views, and emotions;
• lower importance of the opinions of others (M = 7,73; SD = 3,723), which may reflect impaired social sensitivity or changes in the evaluation of interpersonal feedback;
• and more feelings of depression in relationships (M = 9,38; SD = 4,499), which may indicate greater emotional vulnerability and the need for targeted psychological support.
These results emphasize the importance of including components of social skills, emotional regulation, and assertiveness training in psychosocial programs for individuals with ABI. Further research should examine the extent to which specific cognitive and neurological consequences of injury contribute to the observed differences and how individualized interventions can improve interpersonal functioning in this population.
The results show that self-esteem in relationships is significantly associated with several psychological and relational factors in both groups, with the correlations being mostly higher in the group of persons with acquired brain injury (ABI), which suggests a slightly different structure of interpersonal psychodynamics in this population.
In both groups, a medium to high positive correlation was found between self-esteem and internal locus of control (cg: r = 0.468**; ABI: r = 0.611**), which means that higher perceptions of self-esteem in relationships are also accompanied by greater conviction of individuals that they have control over what happens in relationships. This relationship is particularly pronounced in persons with ABI, which could indicate the importance of rehabilitation aimed at restoring a sense of internal control and personal efficacy in relational situations.
Similarly, relationship awareness (EG: r = 0.470**; ABI: r = 0.618**) coincides with a greater introspective ability to understand the dynamics of partner relationships. This may indicate that individuals with ABI, despite neurological damage, maintain (or compensatorily develop) the ability to reflect on relationships when they have developed higher self-esteem.
Assertiveness in the relationship was most strongly associated with self-esteem in both groups (KS: r = 0.596**; PMP: r = 0.759**). This association is particularly pronounced in individuals with PMP, which supports the thesis that a sense of personal worth is crucial for the ability to clearly and confidently express emotions, needs, and boundaries. In these individuals, assertiveness can fluctuate greatly, depending on how stable and positive they experience themselves as a partner.
Perceived relationship satisfaction is also significantly positively correlated with self-esteem (CS: r = 0.546**; PMP: r = 0.606**).
Also interesting is the result for the dimension of desire for a relationship, which is not statistically significant in KS (r = 0.360), but becomes significant in ABI (r = 0.612**). This can be interpreted as a greater dependence of the desire for a partner relationship on self-esteem in people with PMP – probably because the injury affects feelings of competence and desirability, which are often a condition for the expressed need for closeness. The only negative correlation was detected between self-esteem and depression in the ABI group (r = -0.377*), while this connection in KS is not statistically significant (r = 0.064).
Interpretation of correlations between preoccupation in the relationship and selected variables in the control group (CG) and persons with acquired brain injury (EG):
Interpretation of correlations between preoccupation in the relationship and selected variables in the control group (CG) and persons with acquired brain injury (EG): The analysis of correlations between preoccupation in the relationship and psychological variables in the group of persons with acquired brain injury (EG) and the control group (CG) showed significant differences in the associations. In persons with ABI, preoccupation in the relationship is statistically significantly positively correlated with internal locus of control (r = 0.529, p < 0.01), awareness of the relationship (r = 0.601, p < 0.01), anxiety in the relationship (r = 0.401, p < 0.01) and external locus of control (r = 0.429, p < 0.01). In the control group, these correlation coefficients are lower and for some variables are not statistically significant (internal locus of control r = 0.353, p > 0.05; relationship anxiety r = 0.262, p > 0.05; external locus of control r = 0.291, p > 0.05), while awareness of the relationship in CG is also significantly correlated with preoccupation (r = 0.470, p < 0.01). An important difference is also represented by the relationship between preoccupation and the importance of the opinions of others: in CG there is a statistically significant positive correlation (r = 0.453, p < 0.05), while in people with ABI there is no correlation (r = -0.050, p > 0.05). This finding suggests that preoccupation in individuals with ABI is not related to the need for validation from others, which may indicate altered patterns of social perception and regulation in partner relationships after injury. These results are consistent with existing research suggesting that brain injury can affect internal perceptions of control, anxiety, and social function, with personal preoccupation possibly increasing due to changes in emotion perception and regulation.
Interpretation of correlations between internal locus of control and selected variables in the control group (CG) and the group of persons with acquired brain injury (EG):
The results of the correlation analysis show that in persons with acquired brain injury (EG), internal locus of control is statistically significantly positively correlated with awareness of the relationship (r = 0.520, p < 0.01) and assertiveness in the relationship (r = 0.487, p < 0.01). This means that individuals with ABI who perceive greater internal control over events in the relationship also show greater awareness of the dynamics of the relationship and are more assertive in communication within the relationship.
In the control group (CG), the correlations between internal locus of control and awareness of the relationship (r = 0.207) and assertiveness (r = 0.210) are weaker and not statistically significant. This may indicate that these constructs are not as strongly correlated in the general population as they are in individuals with ABI.
The increased association of internal locus of control with mindfulness and assertiveness in the ABI group may indicate the importance of perceived self-control as a protective factor that supports more conscious and active management of partner relationships in this population.
Interpretation of correlations between relationship anxiety and selected psychological variables in the control group (CG) and the group of persons with acquired brain injury (EG)
The results of the correlation analysis show that in the control group (CG), relationship anxiety is strongly and statistically significantly negatively correlated with assertiveness (r = -0.532, p < 0.01) and relationship satisfaction (r = -0.576, p < 0.01). This means that higher levels of relationship anxiety correlate with lower assertiveness and lower relationship satisfaction in individuals without brain injury. In persons with acquired brain injury (EG), however, these negative relationships are weaker and not statistically significant (assertiveness r = -0.105; satisfaction r = -0.302, both p > 0.05).
In both groups, relationship anxiety is strongly positively correlated with depression (CG: r = 0.617**, EG: r = 0.534**), external locus of control (CG: r = 0.613**, EG: r = 0.629**), and fear of relationships (CG: r = 0.516**, EG: r = 0.752**), with the association between anxiety and fear of relationships being more pronounced in the EG.
Interpretation of correlations between assertiveness in a partner relationship and selected psychological variables in the control group (CG) and the group of people with acquired brain injury (EG)
In the control group (CG), assertiveness in a partner relationship is statistically significantly negatively correlated with depression (r = -0.408, p < 0.01) and fear of relationships (r = -0.405, p < 0.01), which means that individuals with a higher level of assertiveness experience fewer depressive symptoms and a lower level of fear in intimate relationships. In addition, assertiveness is positively correlated with relationship satisfaction (r = 0.408, p < 0.01).
In persons with acquired brain injury (EG), a strong negative correlation between assertiveness and depression (r = -0.490, p < 0.01). However, the correlation between assertiveness and fear of relationships is weaker and statistically insignificant (r = -0.222). There is a strong positive correlation between assertiveness and relationship satisfaction (r = 0.684, p < 0.01), which emphasizes the role of assertiveness in the subjective assessment of the quality of partner relationships in persons with ABI. Unlike the control group, assertiveness in the EG group is also positively correlated with the perceived importance of the opinions of others (r = 0.400, p < 0.05).
The analysis of correlations between depression in a partner relationship and selected psychological variables shows that in the control group (CG), depression in a relationship is statistically significantly positively correlated with external locus of control (r = 0.536, p < 0.01), importance of others’ opinions (r = 0.406, p < 0.05), and fear of relationships (r = 0.455, p < 0.05). This means that individuals who attribute control to external factors to a greater extent value the opinions of others and experience more fear of relationships, as well as experiencing more symptoms of depression. At the same time, depression is negatively correlated with relationship satisfaction (r = -0.348, although not statistically significant), which suggests that higher depression coincides with lower satisfaction in partner relationships.
In individuals with acquired brain injury (ABI), depression in a relationship is also positively correlated with fear of relationships (r = 0.505, p < 0.01), indicating the important role of fear as a factor that increases psychological problems in intimate relationships. However, the correlation between depression and external locus of control (r = 0.470) and between depression and the importance of others’ opinions (r = -0.114) was not statistically significant). Depression in this group is strongly negatively correlated with relationship satisfaction (r = -0.672, p < 0.001).
Relationship awareness of people with ABI positively correlates with the dimensions of desire for relationships (r= , 619**), when people with PMS think a lot about relationships and want to stay or be in a partner relationship), with assertiveness (r= , 477**), people are decisive in relationships and with satisfaction (r= , 512**), when they express their opinion in relationships. External locus of control is associated with fear of relationships in both groups (rEG= , 584**, rCG= , 366*). Fear of relationships in EG also correlates negatively with satisfaction with relationships (r= 0.471), in ES the correlation is not statistically significant.
Hypothesis 3:
Persons with ABI feel more loneliness than control group.
The group of people with ABI and CG differ on average in the level of loneliness, but the difference is not statistically significant.
Despite the fact that EG has a small social network, they are not lonely.
Long-term and comprehensive rehabilitation programs are an important protective factor (they prevent the isolation of people with ABI and have a significant impact on the quality of life of persons with ABI.
The group of people with ABI and CG differ on average in the level of loneliness and the size of the social network. People with ABI reported a higher level of loneliness than the control group, but not statistically significant. Therefore, we reject the hypothesis. The results of this study are not consistent with the results of previous studies, as it has already been established that people with ABI are lonelier compared to the general population (Byrne et al., 2022; Kumar et al. 2020; Salas et al., 2022, in Maglica, 2023). Loneliness is rarely considered a problem in rehabilitation after PMP. It is a long-term consequence of ABI.
Even though EG have a small social network (SSQN) with which they are basically statistically significantly satisfied, and they do not feel lonely (rEG=.060; p=0.381). In the process of long-term and comprehensive rehabilitation, people with PMP have a rich network of social contacts (professionals, volunteers, students) and high-quality professional social support. Long-term and comprehensive rehabilitation programs are an important protective factor, preventing loneliness in people with PMP and significantly affecting the quality of life of people with ABI.
In CG, loneliness (UCLA) correlates positively with anxiety in relationships (r=.365; p = <.005) and negatively with assertiveness in relationships (r= -.592, p = <.001).
Even if people with ABI are in a relationship, they do not express their desires and needs and as a result may feel lonely, they lack company, and they do not have common interests with the people around them.
Anxiety correlates with an external locus of control, when the person perceives that they do not have to influence the relationship, which increases anxiety.
During rehabilitation, the social roles of people who have suffered brain injury also change. Related to the rehabilitation process, focused work on everyone, monitoring, individual planning and evaluation.
Social roles in the process of long-term and comprehensive rehabilitation on the formal level remain, but on the experiential level they change and change:
| Formal role | Experiental role | Result | Feelings and states inside of a person after an acquired brain injury (+/-) |
| parent | Children become caregivers – companions, for arrangements for daily life activities, leisure activities, medical care, supervision of drug therapy, help with intimate tasks – toilet | Subordination, impact on socio-economic status | Shame, feelings of guilt, helplessness |
| siblings | Other siblings, taking care of a person with acquired brain injury can be in all areas of a person’s functioning. | They take over the role of a guardian, lose the role of a child | Jealousy, envy, disappointment, anger |
| child | The adult child is placed in the role of a person who is not capable of living independently. | Extended childhood into adulthood, dependency | Trapped in the primary family, Helplessness in achieving independence, Unfinished developmental tasks |
| partner | A healthy partner takes on most of the roles in the relationship (taking care of finances, joint activities, leisure, household, etc.), sexual intimacy | Subordination, dependence, relationship breakdown | Possessiveness, jealousy |
| employee | On sick leave, retired, employed in an adapted workplace or in a disability enterprise | Loss of career, change or loss of professional identity; Becoming a nuisance for the employer, Impact on socio-economic status | Uselessness, Feelings of failure attributed to others, |
| Active in interest groups (recreational athlete, hiker, firefighter, singer, coach, …) | Normally complete loss and halt to previous activities | reconnecting (Center Korak) | Exclusion, Rejection, Incompetence |
| friend | Loss of equal standing in a relationship | Social isolation, reduced social network, loss of previous friendships | Loneliness, Feeling rejected |
| Pearson with car driving licence | Driving with restrictions, loss of driving licence | Negative impact on (in particular) male identity, mobility dependency, reduced independence, reduced social network/loss of social network | Feelings of injustice, anger, helplessness, frustration, feelings of inadequacy |
| Student | A major influence on future life, finding a new identity | Unsuccessful in the mission to continue studies, discontinuation of studies | helplessness |
Conclusion
Rehabilitation of a person with acquired brain injury is a long-term and dynamic process that requires constant adaptation of both the individual and their social environment. The success of rehabilitation depends not only on the scope and quality of therapeutic interventions, but also to a large extent on the quality of social and appropriate professional support available.
Family members often take on an important role in maintaining the daily functioning of the injured person, while at the same time they themselves face significant psychosocial burdens that require appropriate professional support from a multidisciplinary team in the process of long-term and comprehensive rehabilitation of persons after acquired brain injury.
The process of recovery from acquired brain injury is often intertwined with important life transitions, such as integration into the work environment, changes in partner and parental roles, and compensation for the new life reality during periods of major personal and social changes.
Therefore, it is essential that rehabilitation approaches are designed holistically with the aim of providing a stable support framework in the process of long-term and comprehensive rehabilitation for the individual and their family.
The changed social roles of persons after acquired brain injury represent one of the key challenges within the same rehabilitation process for professional complications and persons with ABI. The loss or transformation of roles, such as the role of employee, partner or independent adult, directly affects motivation, participation in rehabilitation and long-term rehabilitation outcomes. Therefore, in the process of long-term and comprehensive rehabilitation, we must recognize social roles as an important rehabilitation factor and systematically include them in the planning and implementation of the rehabilitation of a person after ABI. Rehabilitation goals must be individualized and focused on the real life roles of the individual, with support in adapting existing roles or creating new ones, in accordance with the capabilities of the person after the injury.
For rehabilitation professionals, altered social roles require greater attention in assessing psychosocial functioning and in monitoring the individual’s insight into their own capabilities and limitations. Involving relatives in rehabilitation is important in this context, especially as part of the rehabilitation process, as it allows for the coordination of expectations, supports the stability of the rehabilitation environment.
At the level of rehabilitation policy, this raises the issue of continuity of rehabilitation, accessibility of long-term rehabilitation treatments and clear professional guidelines that define social roles as a legitimate and necessary rehabilitation area. Directing resources into a structured rehabilitation program that systematically addresses the consequences of altered social roles can contribute to a better functional outcome and greater efficiency of rehabilitation of people after acquired brain injuries.
References:
- Abramson, L. Y., Seligman, M. E. P., & Teasdale, J. D. (1978). Learned helplessness in humans: Critique and reformulation. Journal of Abnormal Psychology, 87(1), 49–74. https://doi.org/10.1037/0021-843X.87.1.49
- Azman. A., Jali, A N., Singh. S.J.P.,Abdullah, Ibrahim, H., M.J. (2020). Family roles, challenges and needs in caring for traumatic brain injury (TBI) family members: a systematic review. Journal of Health Research. 34(6), 495-504. Emerald Publishing Limited, DOI 10.1108/JHR-07-2019-0138.
- Braine, M. E. (2011). The Experience of Living with a Family Member with Challenging Behavior Post Acquired Brain Injury. Journal of Neuroscience Nursing, 43(3), 156–164. doi: 10.1097/jnn.0b013e3182135bb2
- Bier, N., Dutil, E., Couture, M. (2009), Factors affecting leisure participation after a traumatic brain injury: an exploratory study. Head Trauma Rehabilitation. 24(3):187-94. DOI: 10.1097/HTR.0b013e3181a0b15a
- Cicerone, K. D., et al. (2011). Evidence-based cognitive rehabilitation: Updated review of the literature from 2003 through 2008. Archives of Physical Medicine and Rehabilitation, 92(4), 519–530.
- Decety, J., Jackson, L.P., (2004). The functional architecture of human empathy. Behav Cogn Neurosci Rev. ;3(2):71-100., DOI: 10.1177/1534582304267187
- Dowing, M., Ponsford, J., (2018)., Sexuality in individuals with traumatic brain injury and their partners. Neuropsychological Rehabilitation. 28(6):1028-1037. doi: 10.1080/09602011.2016.1236732
- Falshaw,L., King, S. N., (2024). Exploring the Role of Social Cognition in Couples’ Relationship Satisfaction and Continuity After Acquired Brain Injury. ResearchGate. DOI:10.31234/osf.io/w846m
- Feuston,J.L., Marshall-Fricker, G.C., Piper, A.M. (2017). The Social Lives of Individuals with Traumatic Brain Injury, Mental Health. May 6–11.
- Goljar, N., (NN). Reintegracija bolnikov po možganski kapi v družbi in na delovnem mestu. https://www.sinapsa.org/eSinapsa/stevilke/20147/102/Reintegracija+bolnikov+po+mo%C5%BEganski+kapi+v+dru%C5%BEbi+in+na+delovnem+mestu
- Hadjam, R. N., Chizanah, L. (2015). The Effect of Traumatic Brain Injury to the Emotional Intelligence. Procedia – Social and Behavioral Sciences 165, 160- 169. https://doi.org/10.1016/j.sbspro.2014.12.618
- Hillier, S. L., Metzer, J. (1997). Awareness and perceptions of outcomes after traumatic brain injury. Brain Injury, 11(7), 525–536. https://doi.org/10.1080/bij.11.7.525.536
- Hammond, M.F., Christine S. D., Whiteside, O.Y., Philbrick P. Hirsch, A. M. (2011). Marital Adjustment and Stability Following Traumatic Brain Injury: A Pilot Qualitative Analysis of Spouse Perspectives. Head Trauma Rehabilitation. Vol. 26, No. 1, pp. 69–78.
- Hoffmann, M., Cases, B.L., Hoffmann, B., Chen, R., (2010). The impact of stroke on emotional intelligence. Bmc neurology 10:103., doi: 10.1186/1471-2377-10-103
- Hynes, C.A., Stone, V.E., Kelso, A.L., (2011) Social and emotional competence in traumatic brain injury: New and established assessment tools, Social Neuroscience, 6:5-6, 599-614, DOI: 10.1080/17470919.2011.584447
- Kreutzer, J., Godwin, E., Marwitz,J., (2010). The truth about divorce after brain injury. Virginia Commonwealth University. https://tbi.vcu.edu/media/tbi/nrc-articles/TruthAboutDivorceWinter2010.pdf
- Kurat T, Goljar N. Kakovost življenja oseb po možganski kapi po zaključeni rehabilitaciji. Rehabilitacija 2009; 8 (1): 9-16.
- Lippincott W., Lippincott Wi. (2011). Interpersonal Relationships and Traumatic Brain Injury. The journal of head Trauma Rehabilitation. 26(1).
- Maglica, P. (2023). Osamljenost in nekateri korelati osamljenosti pri osebah s pridobljeno možgansko poškodbo. Magistrsko delo. Oddelek za psihologijo. Univerza v Ljubljani.
- Morton, M. V., Wehman, P. (1995). Psychosocial and emotional sequelae of individuals with traumatic brain injury: A literature review and recommendations. Brain Injury, 9(1), 81–92., DOI: 10.3109/02699059509004574.
- Nicholas, L. J., Kosciulek, J., (2014). Social interactions of individuals with traumatic brain injury. Journal of Rehabilitation, 80 (2).
- Nochi, M. (1998). “Loss of self” in the narratives of people with traumatic brain injuries: A qualitative analysis. Social Science & Medicine, 46(7), 869–878.
- Northcott, S., Moss, B., Harrison, K. in Hilari, K. (2015). A systematic review of the impact of stroke on social support and social networks: Associated factors and patterns of change. Clinical rehabilitation, 30(8), 811–831. https://doi.org/10.1177/0269215515602136.
- Oddy M. (2001) Sexual relationships following brain injury, Sexual and Relationship Therapy, (16:3, 247-259.
- Ownsworth, T., Haslam, C. (2006). Impact of rehabilitation on self-concept following traumatic brain injury: An interpretative meta-synthesis. Neuropsychological Rehabilitation, 16(4), 489–522. https://doi.org/10.1080/09602010500288865
- Paterson, J., Stewart, J. (2002). Adults with Acquired Brain Injury: Perceptions of Their Social World. Rehabilitation Nursing, 27(1), 13–18. doi:10.1002/j.2048-7940. 2002.tb01973.
- Perlesz, A., Kinsella, G., Crowe, S. (1999). Impact of traumatic brain injury on the family: A critical review. Rehabilitation Psychology, 44(1), 6–35. https://doi.org/10.1037/0090-5550.44.1.6
- Ponsford, J., Sloan, S., & Snow, P. (2013). Traumatic brain injury: Rehabilitation for everyday adaptive living. Psychology Press.
- Radojnič Mhilič, V., (2009). Trenutek, ki spremeni življenje. Spremembe duševnosti po možganski kapi. Inštitut Republike Slovenije za rehabilitacijo. https://www.zdruzenjecvb.com/pdf/publikacija_trenutek_po_ak.pdf
- Rigon, A., Duff C. M., Beadle, J. (2018). Lonely But Not Alone: Neuroticism Mediates the Relationship Between Social Network Size and Loneliness in Individuals With Traumatic Brain Injury, Journal of the International Neuropsychological Society, October 2018, 00,1–8.; DOI: https://doi.org/10.1017/S1355617718001108.
- Rodger, L.L., Williams C., Williams W., (2008). Inabilitiy to empathize following traumatic brain injury. Journal of the International Neuropsychological Society 14(2):289-96. DOI: DOI: 10.1017/S1355617708080326.
- Sander, M.A., Caroselli, S.J., Walter, M., H. jr., Becker, C., Neese, L., Scheibel, R., (2002)., Relationship of family functioning to progress in a post-acute rehabilitation programme following traumatic brain injury. Brain injury, 16(8), 649±657, DOI: 10.1080/02699050210128889.
- Sander, A.M., Struchen, M.A., (2011). Interpersonal Relationships and Traumatic Brain Injury. Journal of Head Trauma Rehabilitation 26(1): p 1-3, January/February 2011. DOI: 10.1097/HTR.0b013e3182068588.
- Salas,E., C., Rojas-Líbano, D., Castro, O., Cruces, R., Evans, J., Radovic, D., Arévalo-Romero, C., Torres, J., Aliaga., Á. (2021). Social isolation after acquired brain injury: Exploring the relationship between network size, functional support, loneliness and mental health. Neuropsychological Rehabilitation, DOI:10.1080/09602011.2021.1939062.
- Sousa de A., McDonald, S., Rushby, J., (2012). Changes in emotional empathy, affective responsivity, and behavior following severe traumatic brain injury., Journal of Clinical and Experimental Neuropsychology., 34:6, 606-623, DOI: 10.1080/13803395.2012.667067.
- Sousa de A., McDonald, S., Rushby, J., Li, S., Dimoska A., James C., (2010). Why don’t you feel how I feel? Insight into the absence of empathy after severe traumatic brain injury. Neuropsychologia. 48: 3585-3595. DOI: 10.1016/j.neuropsychologia.2010.08.008.
- Stenberg,M., Stålnacke B-M., Saveman, B.I., (2020): Family experiences up to seven years after a severe traumatic brain injury–family interviews, Disability and Rehabilitation, DOI: https://doi.org/10.1080/09638288.2020.1774668.
- Segal, D. (2010). Exploring the Importance of Identity Following Acquired Brain Injury: A Review of the Literature. International Journal of Child, Youth and Family Studies, 1(3/4), 293-314. https://doi.org/10.18357/ijcyfs13/420102093
- Sander A. M., Maestas K. L., Pappadis M. R. (2012) “Sexual functioning 1 year after traumatic brain injury: findings from a prospective traumatic brain injury model systems collaborative study,” Archives of Physical Medicine and Rehabilitation, 93 (8), pp. 1331–1337.
- Segev, E., Levinge, M., Hochman, Y., (2018). “Shared Destiny”: The Dynamics of Relationships in Families of Patients with Brain Injury Qualitative Health Research.2018, Vol. 28(1) 112–125, https://doi.org/10.1177/104973231773731.
- Šešok,S., Meško, T., Remšak, T., (2015). Kognitivna oškodovanost, spremembe čustvovanja in motnje razpoloženja v procesu okrevanja po možganski kapi. Akutna možganska kap, Portorož.
- Tičar S., Ristič E. (2022). Changes In Partnership and Sexuality in Persons with Acquired Brain Injury (ABI). Kosmos Publisher, DOI: 10.37722/APHCTM.2022404
- Vešligaj Damiš, J. in Korošec, M., (2019) Pridobljene možganske poškodbe: Dolgotrajna rehabilitacija oseb s pridobljeno možgansko poškodbo v doživljenjskem obdobju; Strokovne podlage za nacionalne smernice in standarde storitev. Maribor: Center Naprej / Center Korak.
- Whiffin C.J., Gracey, F., Ellis-Hill, C., (2021). The experience of families following traumatic brain injury in adult populations: A meta-synthesis of