Therapeutic Decision-Making According to The Phenotypic Pictures of Allergic Patients
Gustavo Machicote Goth*
DVM – MSC – Acred. AVEPA
DOI: 10.37722/AOVSAR.2026102
Endotypes
Disease mechanisms are determined by biomolecular factors, genetics, and environmental interactions, leading to individual differences in expression.
In allergies there are as many combinations of endotypes as there are individuals suffering from the disease.
Patients express their clinical conditions as phenotypes, which are the result of the combination of the endotype and its interaction with the environment
Watch the Article in Motion
Canine Allergic Phenotypes
- Involvement in the armpits and groin with erythema and excoriations
- Pododermatitis with erythema and licking/nibbling
- Pinna erythema and itching with shaking
- Coat conditions, mainly alopecia and seborrhoea
- Blepharitis and cheilitis with erythema and itching
- Gastroenteritis – anal pruritus
Feline Allergic Phenotypes
- Miliary dermatitis in the back and spine
- Head and neck dermatosis.
- Self-induced alopecia
- Eosinophilic complex
- Pigmented urticaria (Eosinophilic Mast Cell Pattern)
- Erythroderma in figures
- Feline asthma
- Gastrointestinal inflammation
- Plasmocitic pododermatitis
Allergies are multifactorial diseases with multimodal, individualized approaches. The better we define the phenotype and its corresponding endotype, the better we can treat the patient.
Diseases That Can Be Confused with Allergies
- Sarcoptic mange
- Epitheliotropic lymphoma
- Presence of fleas
- Pemphigus complex
- Furunculous dermatophytosis
- Itching from other undetected parasites
- Hormonal folliculitis
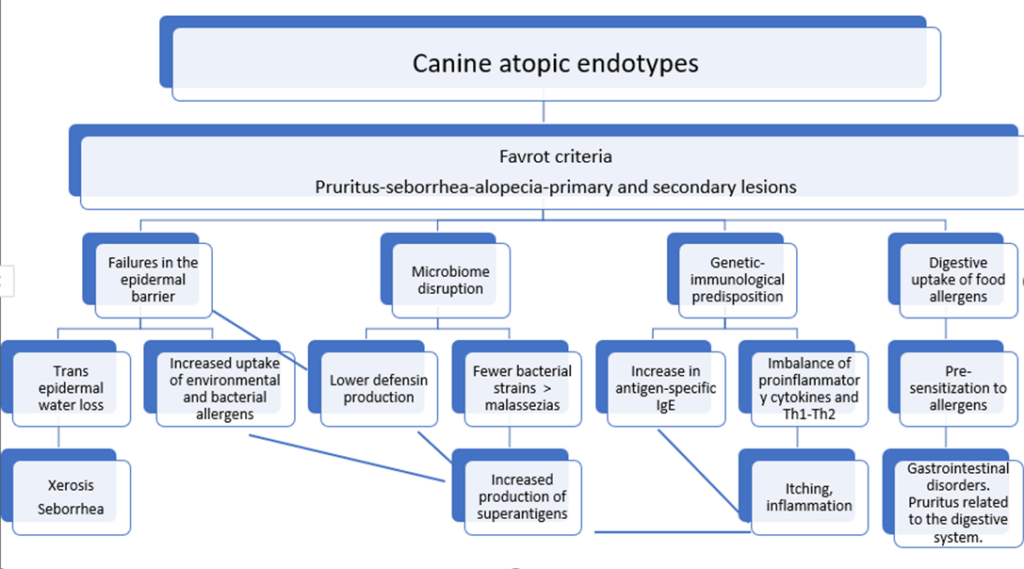
Predominant Clinical Conditions in Dogs:
Endotypic mechanisms
Digestive sensitization
When to be suspicious?
- Itching in areas related to the digestive system.
- Anal Sac Impaction
- Borborygmus – More than 3 stools/day – Variable stool consistencies
- History of previous severe gastroenteritis
- Otitis as the only manifestation
- Response to specific diets including also in perianal fistulas – colitis – onychodystrophies.
- Frequent urticaria and angioedema
- Patients starting at less than 6 months or more than 6 years.
Considering cross-reactions in different foods
- Milk of different species
- Eggs of different birds
- Different fish. Less allergenic blues
- Shellfish and dust mites/storage
- Meat and milk from nearby species
- Soy and other legumes
- Insects and dust mites
- Ruminants
- Swine
- Environmental allergens can enter through the digestive tract.
Statistically, it has been shown that the most frequent food allergens in descending order in dogs are beef, dairy, chicken, wheat and lamb. (Mueller, Olivry, & Prélaud, 2016).
Cats can also suffer purely immunological adverse reactions to food, which is why it is correct to call them food allergies (Halliwell et al, 2021), more frequently against allergens from cattle, fish and lamb (Mueller, Olivry, & Prélaud, 2016)
And how do we manage this problem?
- Blocking the symptoms
- Avoiding the trigger protein if we know it.
- Avoid this protein in general, providing hydrolyzed foods or novel proteins.
Alteration Of the Skin Microbiome
Why does it occur?
- Defects in the epidermal barrier
- Poor synthesis of defensins
- Cutaneous xerosis
- Pro-inflammatory cytokines that promote dysbiosis due to scratching and inflammation
- Shortages of a variety of bacterial strains
When do we suspect an alteration of the microbiome?
- Recurrent dysbiosis
- Recurrent seborrheic dermatitis – Collarets
- Recurrent superficial and deep pyodermas
- Recurrent otitis, sometimes only with overgrowth
And how do we manage this problem?
- Improving the skin barrier
- Shampoo therapy
- Pre-pro-postbiotics
- Avoiding unnecessary skin aggression
- Immunomodulators
- Domperidone
- Beta-glucans
- Nucleotides
- AHCC. Promoter of T-cell differentiation to Th1 (Lentinus Edodes, fungus)
- Lokivetmab
- Keratinocyte stabilizing immunomodulators (TSLP)
Th1 Th2 immune reactive imbalance
- Genetically these individuals deviate in the production of IgE and IgG in general, although, some individuals would have a more Th1 alteration and could be the so-called atopic like.
- Genetic imbalance that diverts the production of inflammatory cytokines and Pruritogenic
When do we suspect this immune imbalance?
- Itching sine materia (primary)
- Initial erythema
- Hyperacute reactions with subcutaneous oedema
- Presence of primary papule-like lesions and secondary excoriations
- Predisposed Breeds and Family History
- Rapid response to corticosteroids, lokivetmab, and oclacitinib/ilunocitinib/atinvicitinib
And how do we manage this problem?
- Interfering with cytokines by deciding the spectrum of the therapeutic molecule according to the degree of inflammation
- Specific or reduced spectrum LOKIVETMAB
- Medium spectrum
OCLACITINIB/ILUNOCITINIB/ATINVICITINIB
- Broad-spectrum fast-acting CORTICOSTEROIDS
- Broad-spectrum slow-acting CYCLOSPORIN
- Eliminate allergens deposited on the skin with baths
- Avoid spreading these allergens
- Immunotherapy
Skin barrier failures
Mechanism Explained
• It has been proven that the presence of cytokines secreted by Th2 lymphocytes increased in atopic cells, specifically interleukins (IL): IL-4, IL-13, IL-25 and IL-33, together with tumor necrosis factor α (TNF-α) and interferon gamma (IFN-γ), are capable of modulating the function of keratinocytes causing an increase in the secretion of thymic stromal lymphopoietin (TSLP), causing pruritus) and induce apoptosis in these cells. This increase in TSLP levels in turn stimulates dendritic cells by increasing Th2 levels and, in addition, causes a decrease in the production of long-chain fatty acids and ceramides esters, altering the skin barrier and, therefore, reducing their effectiveness in terms of the defence mechanism against external agents. The increase in Th2 lymphocytes in the dermis induces the formation of serine protease 7 kallikrein, which, at high levels, also participates in the dysfunction of the epidermal barrier. (Weidinger and Novak, 2016)
When do we suspect this failure?
- Gross skin modification
- Xerosis
- Lichenification
- Hyperpigmentation
- Peeling
- Secondary dysbiosis. Rancid smell
- Hirsute hair
- Response to Supplements and Hydration
And how do we manage this deficiency therapeutically?
Oral supplementation
- Quality nutrition
- Capsules
Topical supplementation
- Spot on
- Collar
- Mousse
- Moisturizing and repairing shampoo therapy.
- Moisturizing lotions
We have tried to simplify and briefly group allergic individuals, mainly dogs, into 4 endotypes.
But it is almost impossible that, with the passage of time, the proportion of these four endotypes does not vary and they become the protagonists of the clinical condition according to the interaction with the environment.
And about cats, what can we say?
- Feline Atopic Syndrome can include skin syndrome, asthma and food allergy.
- That is evident that the three key processes associated with Feline Atopic Syndrome—namely, skin syndrome, asthma, and food allergy—appear to share a notable involvement of immunoglobulin E (IgE). This suggests that IgE plays a significant and common role across these manifestations, contributing to the underlying pathophysiology observed in affected cats.
- That their phenotypes are very different from the dog because other proportions of cytokines possibly act
- That eosinophils play a leading role (IL3 and 5), due to their collagenolytic enzymes and their scratching tool, which is mainly the tongue.
- That stress seems to be more important in the development and aggravation of the disease than in dogs
- That their microbiome does not seem to alter so much as to produce frequent dysbiosis. However, he would function as a sentinel. (Older, Caitlin E., et al. Characterization of staphylococcal communities on healthy and allergic feline skin. Veterinary dermatology, 2021, vol. 32, no 1, p. 61-e10)
- The skin structure may also have integration defects in allergy sufferers, although less is known.
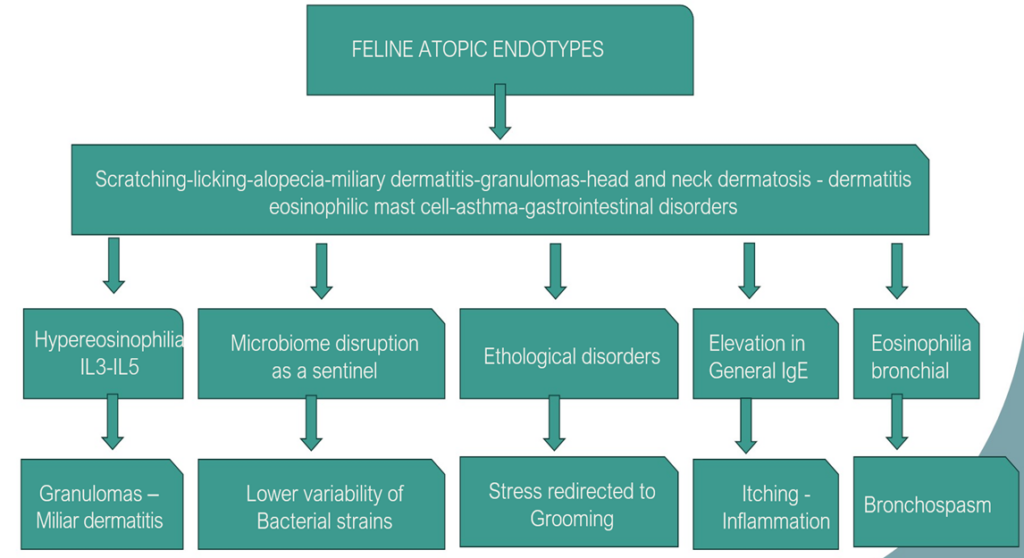
Feline Atopic Endotypes/Phenotypes
The most frequent phenotypes can be:
- Scratching
- Licking
- Alopecia
- Miliary dermatitis
- Granulomas and plaques
- Head and neck dermatosis.
- Eosinophilic mast cell dermatitis
- Asthma
- Gastrointestinal disorders
- Ulcerative dermatitis and alopecia of neuropathic origin
- Plasmocitic pododermatitis
Endotypic Mechanisms in Cats
In dogs and cats, depending on the phenotypic expressions, we can choose individualized treatments.
Relationship between clinical pictures, endotypes and immunomodulatory therapeutic management in dogs
And what is the reason for these different choices?
Inhibitors of receptors or cytokine itself:
Broad spectrum:
• Corticosteroids
• Cyclosporine – calcineurin inhibitor – Inhibition of mRNA and enzymes
Intermediate Spectrum:
• JAK inhibitors: oclacitinib, ilunocitinib, and atinvicitinib
• TNF-alpha inhibitors and mast cell degranulation such as palmitoylethanolamide
Specific spectrum:
• Monoclonal antibodies: lokivetmab (IL31)
• P-substance blockers (Maropitant)
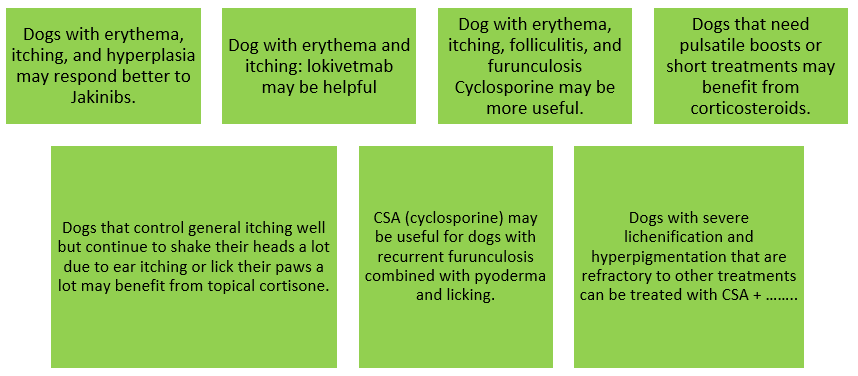
Summary of Some Examples of Therapeutic Strategies According to Phenotype of dogs and cats:
- Dog with erythema and occasional itching of 6 months of age: LOKIVETMAB OR ATINVICITINIB.
- Dog with erythema and itching extended over time with more than one year: JAKINIBS – LOKIVETMAB – SKIN BARRIER IMPROVERS.
- Dog with moth-eaten dysbiosis and itching 4/10: SHAMPOO-PROBIOTICS- REPAIR BARRIER.
- Dog with furunculosis and frequent licking, mainly in bony protrusions: CYCLOSPORINE – SHORT-TERM CORTICOSTEROIDS – BENZOYL PEROXIDE SHAMPOO.
- Dog with 8/10 pruritus, hyperpigmented, lichenified skin and xerosis: JAKINIBS, ANTIMICROBIALS – BARRIER CORRECTORS – HYDRATION.
- Dog with recurrent otitis and a lot of itching in the mouth and anus: ELIMINATION DIET – LOKIVETMAB – JAKINIBS.
- French Bulldog dog, with erythema, seborrhoea, pododermatitis and otohematomas scars: JAKINIBS – SHORT-TERM CORTICOSTEROIDS OR LONG-TERM CYCLOSPORINE.
- Cat with facial and neck dermatosis pattern. Pruritus 10/10: ELIMINATION DIET – DEXAMETHASONE – LONG-TERM CYCLOSPORINE.
- Cat with miliary dermatitis on the back: ISOXAZOLINE – PREDNISOLONE – CYCLOSPORINE.
References:
- Miller, William H., Craig E. Griffin, and Karen L. Campbell. Muller and Kirk’s small animal dermatology. Elsevier Health Sciences, 2012.
- Santoro, Domenico, et al. Pathogenesis of canine atopic dermatitis: skin barrier and host–micro‐organism interaction. Veterinary dermatology, 2015, vol. 26, no 2, p. 84-e25
- Marsella, R. (2021). Advances in our understanding of canine atopic dermatitis. Veterinary Dermatology, 32(6), 547-e151.
- Gedon, N. K. Y., & Mueller, R. S. (2018). Atopic dermatitis in cats and dogs: A difficult disease for animals and owners. Clinical and Translational Allergy, 8, 41. doi: 10.1186/s13601-018-0228-5
- Halliwell, R., Pucheu-Haston, C. M., Olivry, T., Prost, C., Jackson, H., Banovic, F., Nuttall, T., Santoro, D., Bizikova, P., & Mueller, R. S. (2021). Feline allergic diseases: Introduction and proposed nomenclature. Veterinary Dermatology, 32, 8–e2. doi: 10.1111/vde.1289.
- Vargo, Cheryl, et al. Characterization of the serum cytokine profile in feline atopic skin syndrome. Veterinary Dermatology, 2021, vol. 32, no 5, p. 485-e133.
- Szczepanik, Marcin P., et al. Evaluation of the correlation between Scoring Feline Allergic Dermatitis and Feline Extent and Severity Index and skin hydration in atopic cats. Veterinary dermatology, 2018, vol. 29, no 1, p. 34-e16.